
Introduction Excretion Excretory Organs And Excretory Products
You throw your household waste every day into the dustbin. Even your body produces different types of waste every day. Have you ever thought about what happens to those wastes? How are they expelled from the body? This work is carried out by the excretory system.
Different types of wastes are produced in the body -through various metabolic processes. For example, proteins present in our diet get metabolized to produce ammonia, ureSÿand uric acid.
Carbon dioxide, produced due to respiration, is also a waste product. These waste products need to be removed from the body.
The organ system, that is responsible for the removal of wastes from our body, is called the excretory system.
Excretory products and their elimination notes for NEET PDF
Different types of excretory products or wastes are produced by the metabolic activities of cells. They are removed from the body by the process of excretion, carried out by the excretory organizer
Exteriors: The biological process by which the metabolic wastes (nitrogenous and other harmful substances) are removed from the body is called excretion.
Excretory organs: The organs responsible for producing, collecting, and removing the metabolic wastes (both nitrogenous and non-nitrogenous) from the body are called the excretory organizer

The organ of the excretory system, that produces most of the wastes is called the primary excretory organ.
The organs that take part in excretion though they have other major roles in the body, are called accessory excretory organisers Kidney is the primary excretory organ in our body, whereas the lungs, salivary glands, skin, liver, and large intestine are accessory excretory organisers
| Class 11 Biology | Class 11 Chemistry |
| Class 11 Chemistry | Class 11 Physics |
| Class 11 Biology MCQs | Class 11 Physics MCQs |
| Class 11 Biology | Class 11 Physics Notes |
Excretory products: The unwanted and harmful substances, generated by metabolic activities in the body, are called excretory products. For example, urea, ammonia, uric acid, etc.
Types of excretory products: Waste products produced are generally of the following types—
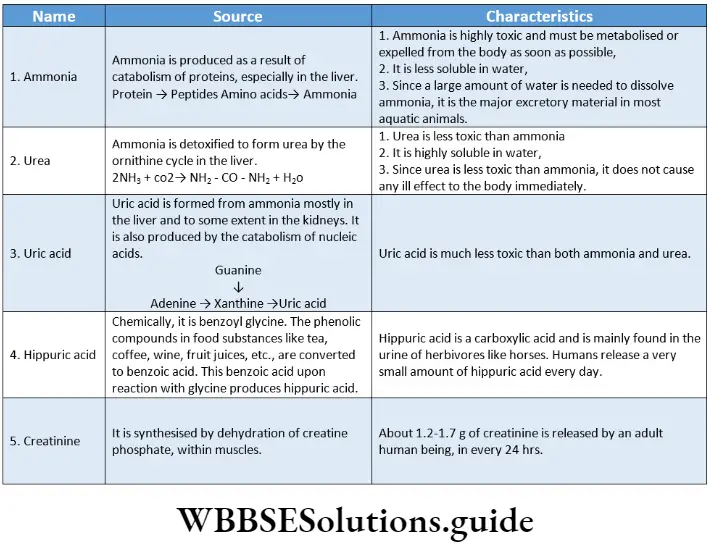
Nitrogenous waste products: These are nitrogen-containing waste products generated by the catabolism of proteins and nucleic acids. For example, ammonia, urea, hippuric acid, etc., are some of the nitrogenous waste products of animals.

Removal of waste products: Like us, unicellular organisms also produce metabolic wastes and toxic compounds. These wastes are excreted directly from the cells, into the external environment.
Multicellular organisms require different excretory organs to remove the wastes. The wastes produced in the body enter the excretory system through different body fluids, such as blood and lymph. Finally, they are removed from the body through the excretory organs as excretory products.
Class 11 biology excretory products and their elimination notes with diagrams
Importance of excretion:
- The harmful metabolic wastes, if not removed may cause several disorders and malfunctioning of different organs of the body. Excretion serves to remove these and helps the body to function properly.
- Excretion also maintains proper metabolic conditions in the cell. It helps to
maintain the concentrations of ions and water within the cells, thus maintaining homeostasis.
Modes Of Excretion In Animals
Depending on the excretory product, there are Different Modes of excretion in animals.
Principal Modes Of Excretion
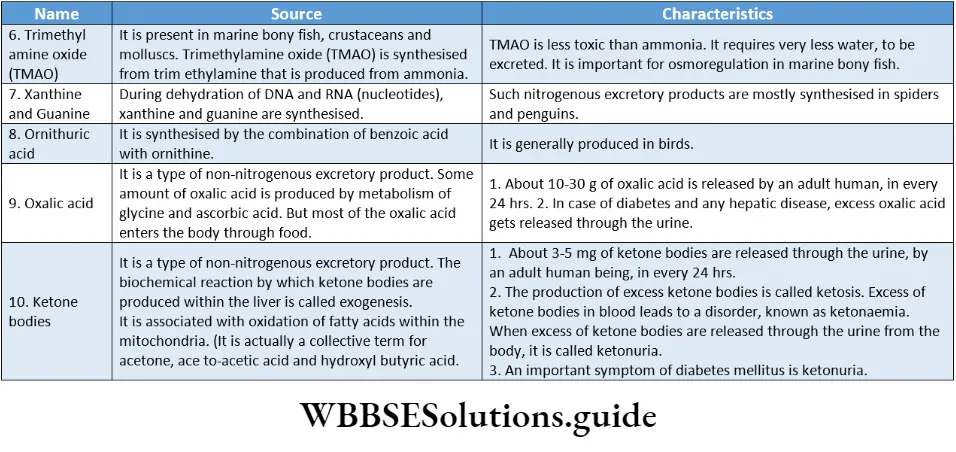
Ammonia, urea, and uric acid are the principal excretory products in animals. Based on the type of nitrogenous wastes released, excretion can be of the following types—
- Ammonotelism,
- Ureotelism and cd uricotelism.
Ammonotelism: The excretion of nitrogenous wastes from the body, mainly in the form of ammonia, is called ammonotelism.
The animals, that release ammonia as the main nitrogenous waste product, are called ammonotelic animals.
For example, aquatic animals like sponges, coelenterates, crustaceans, cnidarians, Platyhelminthes, echinoderms, bony fish, tadpoles, salamanders, etc.
Ureotelism: The excretion of nitrogenous wastes from the body, mainly in the form of urea, is called ureotelism.
The animals that excrete urea as the main nitrogenous waste are called ureotelic animals. For example, man, whales, desert mammals like kangaroo rats, camels, terrestrial amphibians, aquatic and semi-aquatic reptiles like alligators, etc.
Uricotelism: The excretion of nitrogenous wastes mainly in the form of uric acid, is called uricotelism.
The animals that excrete uric acid as the main nitrogenous waste product are known as uricotelic; animals. For example, birds, land reptiles, insects, land snails, and some land crustaceans, etc.
Dual Excretion
Some of the ammonotelic organisms can become partially ureotelic under adverse conditions, especially at times of shortage of water in the environment and in the organism’s body.
For example, Earthworms, when present in moist soil, release ammonia as the excretory product, but release urea, when present in dry soil.
Other Modes Of Excretion
Besides the principal modes of excretion, there are some other modes of excretion as well. They are as follows—
Aminotelism: The excretion of excess amino acids, without being converted to any other substance, is called aminotelism.
Animals showing this mode of excretion, are called aminotelic animals. Some members of Phylum Mollusca and Echinodermata are amniotic.
Guanotelism: The excretion of guanine as the main nitrogenous waste product is called guanotelism.
Animals showing this mode of excretion are called guanotelic animals. Spiders, some bony fish, and some members of Phylum Mollusca are guanotelic.
Short notes on excretory products and their elimination for quick revision
Excretory Organs Of Invertebrates
The excretory system in different organisms varies according to their complexity.
It shows the process of evolution from simple to complex organisms. Freshwater and terrestrial invertebrates have a wide variety of adaptations for maintaining salt and water balance (osmoregulation), and also excreting nitrogenous wastes.
Three well-known invertebrate excretory organs are—protonephridia, metanephridia, and Malpighian tubules.
Protonephridia and flame cells: The tubular excretory structures of Platyhelminthes (flatworms) are called protonephridia. It contains specialized excretory cells called flame cells.
Also found in rotifers, some annelids, and the cephalochordata—Amphioxus/ Branchiostoma.
Nephridia: The simple tubular excretory structure, usually found in annelids, is called nephridia. It removes nitrogenous wastes and maintains a fluid and ionic balance in the body.
Malpighian tubules: The tubular excretory structure of insects is called Malpighian tubules.
Green glands: Green glands or Antennal glands remove excretory products in crustaceAnswer:
Human Excretory System
Human Excretory System Definition: The organ system that is responsible for collecting and removing the metabolic wastes from the human body is called the human excretory system.
The human excretory system consists of a pair of kidneys, a pair of ureters, the urinary bladder, and the urethra.
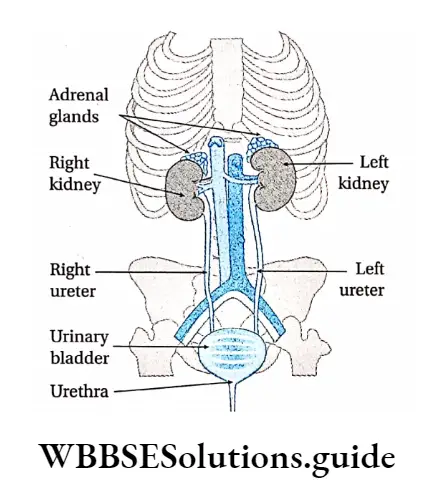
Kidneys
Kidneys Definition: The pair of bean-shaped organs, located in the abdominal cavity, that are responsible for the production of urine are called kidneys.
Kidney Location: The kidneys are located near the rear wall of the abdominal cavity.
They are considered retroperitoneal, which means they lie behind the peritoneum.
Each kidney extends between the 12th thoracic vertebra and the 3rd lumbar vertebra, on both sides of the backbone. The right kidney is situated a little lower than the left kidney.
Kidneys Shape And Size: Each kidney measures about 10-12 cm in length, 5-6 cm in breadth, and 3-4 cm in thickness. The right kidney is slightly smaller than the left one.
Kidneys Weight: The kidney usually weighs 120-170 g. In healthy adult males, each kidney weighs an average of 170 g while in healthy adult females it weighs around 135 g.
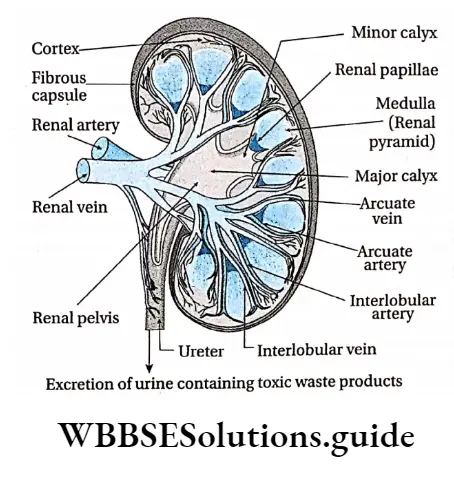
Kidneys Structure: Each kidney is covered with a tough capsule made up of fibrous connective tissue. It is known as the renal capsule. The renal capsule is surrounded by a layer of fat, the adipose capsule, and another outer fibrous membrane, the renal fascia.
Adhering to the surface of each kidney, there is a layer of fat (pararenal fat) that protects the kidney from mechanical shock. One side of the kidney is concave in nature. This region has a depression, where renal artery enters while the renal vein and ureter exit the kidney.
This depression is called the hilum. The longitudinal section of a kidney shows three distinctive layers. The outer, granulated layer is called the renal cortex.
Excretory products and their elimination chapter summary with important points
It stretches down through a radially striated middle layer. It is called the renal medulla. A hollow cavity, called the renal pelvis, connects the kidney to the ureter, through which urine passes to the urinary bladder.
The renal pelvis branches into 2-3 compartments, inside the kidney. These are called major calyces (singular: calyx).
The major calyces are further divided into smaller compartments, called minor calyces. The renal medulla is divided into 8-18 triangle-shaped compartments, called renal pyramids.
Several renal pyramids join to form the renal papilla. The renal cortex extends into the renal medulla between the renal pyramids, forming long column-like structures, called renal columns of Bertin.
The kidneys are made up of several tubular structures called nephrons. According to their location, nephrons may be—superficial or cortical and juxtamedullary.
Each nephron is made up of the following parts—Malpighian corpuscle and Renal tubule.
Several renal tubules from adjacent nephrons join to form a larger tubule, called collecting tubule.
These are generally found in the renal medulla. This makes the medulla appear striated. Several collecting tubules join further to form the ducts of Bellini.
Kidneys Functions: Kidneys in the human body carry out Serval important Functions. They Are-
Kidneys Formation of urine: The primary function of the kidneys is to produce urine. Several nitrogenous and non-nitrogenous wastes get excreted from the body Through urine. urine is actually produced within the Nephrones Present in the kidneys.
Kidneys Maintenance of concentration of H+ and other inorganic ions in blood: Kidneys help to maintain the pH of the blood by releasing hydrogen (H+) ions and reabsorbing bicarbonate (HCO3–) ions.
They also play an essential role in regulating the amount of several important inorganic ions in the body. These include Na+, K+, C–, HCO–3,H+,Ca2+ And PO43-.
Kidneys Maintenance of plasma volume: Kidneys help in the absorption of Na+ ions as well as water. This helps to maintain the volume of plasma.
Kidneys Reabsorption: The nephrons selectively reabsorb certain important ions as well as water. This helps to maintain the proper concentration of ions in the blood.
Kidneys Removal of wastes and harmful substances: Wastes such as ammonia, urea, uric acid, hippuric acid, etc., that are generated within the body, get excreted through urine. Besides these, several other harmful substances such as toxins, drugs, etc., also get removed from the body by urine.
Kidneys Maintenance of acid-base balance in the body: Another important role of the kidneys is the regulation of acid-base balance. Many of the metabolic functions in the body are sensitive to pH.
Thus, the pH of the body fluids must be maintained within a narrow range. This function is carried out by the coordinated action of the lungs, liver, and kidneys.
Controlling blood pressure: The kidneys produce an enzyme, called renin. When the blood decreases, this enzyme is secreted. This enzyme activates the renin-angiotensin system.
This constricts blood vessels and helps to increase blood pressure. It also helps in the absorption of Na+ ions as well as water. This influences the plasma volume.
It again influences the total blood volume, which in turn regulates blood pressure.
Production of RBCs: Kidneys secrete a hormone called erythropoietin in response to low oxygen levels in tissues Erythropoietin stimulates red blood cell formation in the bone marrow. Decreased erythropoietin secretion leads to low erythrocyte production which may cause anaemia.
Homeostasis: Kidneys are able to maintain homeostasis by varying the concentration of urine. They reabsorb water and ions from urine when blood plasma volume is low.
They do not reabsorb ions and water from urine (hence, producing dilute urine) when blood plasma volume is high. This regulates the water content in the blood, which in turn maintains homeostasis.
Secretion of different substances: Kidneys also serve as important glands that secrete renin, calcitriol, erythropoietin, etc.
Renin activates the renin-angiotensin-aldosterone system, which helps to regulate blood pressure and sodium-potassium balance.
Calcitriol, on the other hand, is a metabolite of vitamin D3. It is necessary for normal reabsorption of Ca2+ by the gastrointestinal tract.
It is also important for the deposition of calcium in bones and the synthesis of collagen tissue. Erythropoietin regulates RBC production in bone marrow.
Ureters
Ureters Definition: The muscular tubes that carry urine from the kidneys to the urinary bladder are called the ureters.
Ureter Location: Each ureter descends downwards from the hilum of each kidney, to enter the urinary bladder posteriorly at its inferior surface.
Ureters Structure: The ureters are muscular tubes about 25 cm long and 30 mm in diameter. The lumen of the ureter is narrow and branched.
Ureters Functions:
Both the ureters transport urine produced in the kidney, from the renal pelvis to the bladder.
Peristaltic contractions by the involuntary muscles, cause urine to enter the bladder.
Excretory Class 11 Notes
Since the ureters pass behind the urinary bladder, and enter the bladder at its base, the bladder compresses the openings of the ureters. This prevents the back-flow of urine into the ureters when pressure in the bladder is high during urination.
Urinary Bladder
Urinary Bladder Definition: The pear-shaped, muscular, sac-like organ that collects the urine and stores it till urination is called the urinary bladder.
Urinary Bladder Location: The urinary bladder is located in the pelvic cavity, just posterior to the pubic symphysis.
In males, it is directly anterior to the rectum. In females, it is anterior to the vag*na and inferior to the uterus.
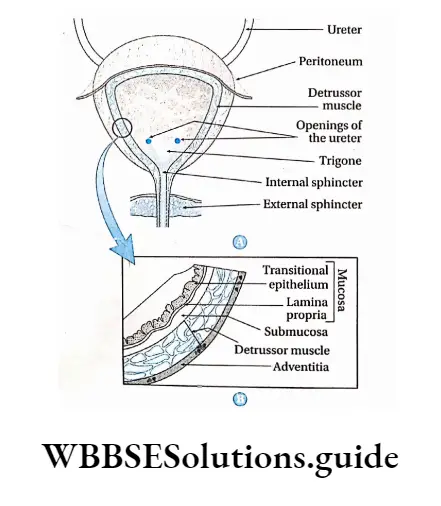
Urinary Bladder Anatomical structure: The urinary bladder is triangular in shape when empty, but appears oval when filled with urine.
It is composed of transitional epithelium. The bladder has three openings—two for the ureters and one for the urethra, which drains out the urine.
The trigone is a smooth triangular area at the base of the bladder bordered by these three openings. Two sphincters are found at the junction of the urethra and the bladder. They are internal and external sphincters.
The internal sphincter is present around the opening of the urethra. Inferior to the internal sphincter, the external sphincter is present. It is composed of skeletal muscle that can be voluntarily controlled. The bladder has several features that allow it to retain urine.
After urine enters the bladder through each ureter, small folds of bladder mucosa act like valves to prevent its backflow.
These folds are made up of transitional epithelial tissues that prevent the reabsorption of urine from the urinary bladder. About 600 ml of urine can be stored in the urinary bladder.
Urinary Bladder Functions: The function of the urinary bladder is to store urine prior to its elimination from the body.
When the urinary bladder gets filled with 300 – 400 ml of urine, an adequate stimulus is generated for its elimination. The bladder then expels urine into the urethra by a process, called micturition.
Urethra
Urethra Definition: The small tube-like structure, extending from the urinary bladder, through which the urine is excreted out of the body is called the urethra.
Urethra Location: It begins at the neck of the urinary bladder and ends at the external urethral orifice.
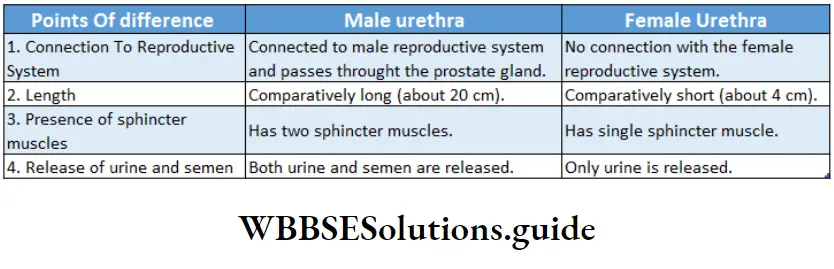
Urethra Anatomical structure: The urethra is a fibromuscular tube that conducts urine from the bladder (and s*men in males) to the exterior. It is different in structure in males and females.
In males, the urethra is about 20 cm in length. It can be divided into 4 parts. The pre-prostatic urethra is about the first 0.5-1.5 cm in length from the internal urethral orifice.
At this orifice a sphincter muscle is present. The next part extends through the prostate gland. This part is called the prostatic urethra.
At this region, the ejaculatory duct (receives sperms) and several prostatic ducts (receives prostate fluid) meet the urethra.
The urethra now passes the external urethral sphincter, through the perineum at an angle of 90°, before entering the penis.
This portion is called the membranous urethra. Then the urethra enters the penis. This portion is called the penile urethra. Urethra opens to the exterior by a small orifice at the apex of the penis which is called urinogenital aperture or urinary meatus.
In males, the urethra carries urine during urination and sperm during ejaculati*n. The female urethra is about 4-5 cm in length. It extends from the internal to the external urethral orifice.
The urethra is fused with the anterior wall of the vag*na. It ends at the urethral orifice or urinary meatus located between the clitor*s and the vag*na.
There is an external urethral sphincter present near this opening. In females, the reproductive and urinary systems are not connected.
Urethra Functions: The urethra serves as the passageway through which urine is discharged from the body. In males, the urethra also serves as the duct through which s*men is ejaculat*d.
Nephron
Nephron Definition: The structural and functional unit of the kidney is called the nephron.
The name ‘nephron’ comes from the Greek word ‘nephros’, meaning ‘kidney’. Each nephron has two parts a globular renal corpuscle or malpighian body and a tubular structure called renal tubule.
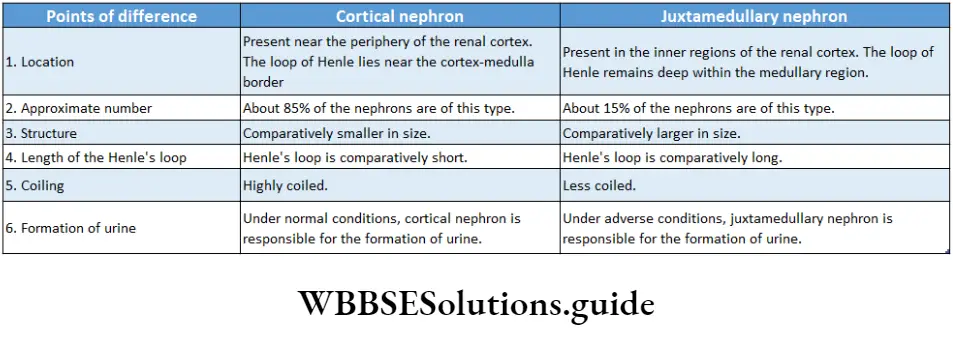
Nephron Location: Most (85%) of the nephrons are present in the renal cortex. The rest (15%) of them are present in the juxtamedullary region of the renal medulla.
Number: Each human kidney has approximately 1.3 million nephrons.
Nephron Types: There are two types of nephrons—
- Superficial and
- Juxtamedullary.
Superficial nephron: The nephron, in which the renal corpuscle remains in the outer region of the cortex and the loop of Henle (a part of renal tubule) is at the outer zone of the medulla, is called a superficial nephron.
This is also called the cortical nephron. About 85% of the nephrons are superficial in nature.
They are mostly located in the periphery of the renal cortex. A few species, including humans, possess very short superficial nephrons whose loop of Henle is short and never enters deep into the medulla.
The efferent arterioles from adjacent nephrons form a network of peritubular capillaries. These are the nephrons that are responsible for the production of urine under normal conditions.
Juxtamedullary nephron: The nephron, in which the renal corpuscle is located in the inner region of the cortex next to the medulla, and the loop of Henle enters the medulla, is called juxtamedullary nephron.
They are generally located in the inner cortex and medulla. They can produce urine during emergency periods.
They differ from superficial nephrons in two important ways—
- The loop of Henle is longer and extends deeper into the medulla.
- The efferent arterioles of adjacent nephrons form not only a network of peritubular capillaries but also a series of vascular loops called the vasa recta around the loop of Henle.
Parts Of Nephron
Nephrons are differentiated into the following regions—
- Malpighian body or renal corpuscle
- Renal tubule.

Malpighian body or Renal corpuscle
Malpighian body or Renal corpuscle Definition: The flattened spherical part of the nephron is called the malpighian body or renal corpuscle.
The Malpighian body is present in the renal cortex only. It has a diameter of about 200 pm.
It consists of a tuft of interconnected capillaries, called glomerulus (plural: glomeruli), that is encased in a hollow sphere called Bowman’s capsule
Glomerulus: A network of capillaries within the Bowman’s capsule that performs ultrafiltration of blood is known as glomerulus.
The afferent arteriole (50 pm in diameter) that leads to the glomerulus has a larger diameter than the efferent arteriole (25 pm in diameter) that leaves it. So the blood pressure in the glomerulus remains very high.
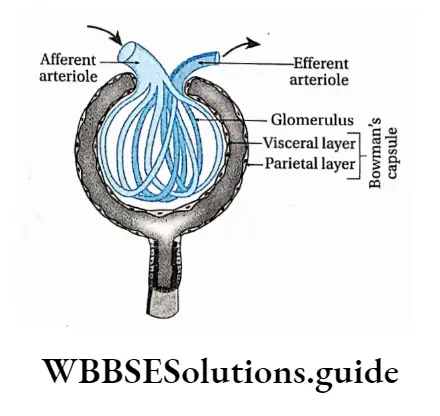
Bowman’s capsule: The hollow, double-layered, cup-shaped part of the renal corpuscle that holds the glomerulus is called the Bowman’s capsule (also called the glomerular capsule)
It is composed of visceral (inner) and parietal (outer) layers
Visceral layer: It is a single layer of squamous epithelium that lies next to the glomerular capillaries. The visceral layer is made of specialized cells, called podocytes.
These podocytes send small projections or foot processes over the length of the glomerulus. The foot processes are called end-feet or pedicels. They interdigitate with one another forming filtration slits.
The size of the filtration slits (generally 25 pm) restricts the passage of large molecules (e.g., albumin) and cells (e.g., RBCs and platelets).
Parietal layer: It lies next to the visceral layer. It is made up of a single layer of simple squamous epithelial cells.
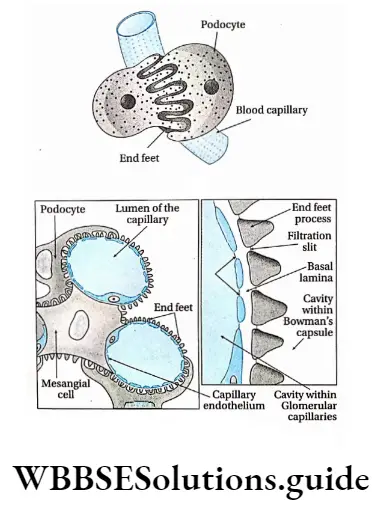
A common basement membrane is present in between the inner layer of the Bowman’s capsule and the endothelium of the glomerulus.
Renal tubule Definition: The tubular part of the nephron, extending from the parietal layer of the Malpighian body, is called the renal tubule.
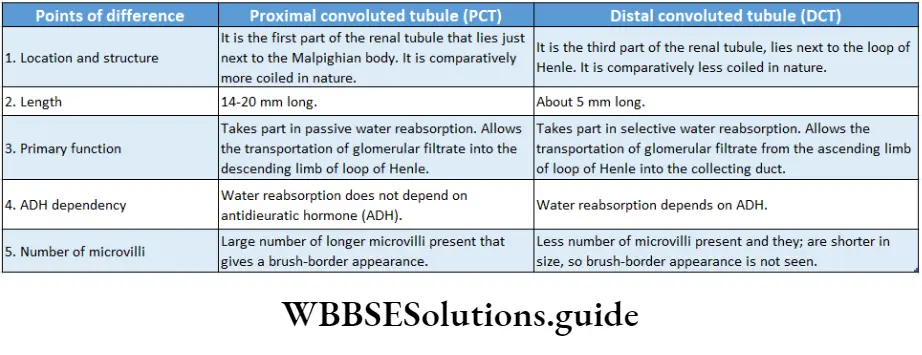
The renal tubule is about 3 cm in length. It has three parts—The proximal convoluted tubule (PCT), a loop of Henle, and a distal convoluted tubule (DCT).
Proximal convoluted tubule (PCT): The longest and the most convoluted part of the nephron is called the proximal convoluted tubule
Proximal convoluted tubule Characteristics:
- It is about 15 mm long and has an external diameter of about 60 mm.
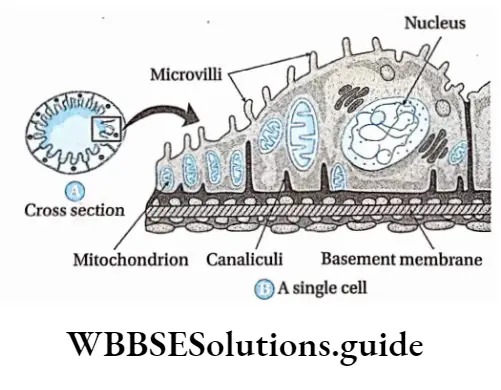
- The walls of PCT are made up of a single layer of closely-placed epithelial cells called podocytes.
- The cells have projections called pedicels or end feet. These cells interdigitate with one another and are united by apical tight junctions (intercellular junctions between adjacent epithelial cells at the apex of the cells).
- The PCT has a layer of cuboidal cells surrounding the lumen.
- The cells, lining the lumen, have numerous finger-like projections from their free ends. These are called microvilli. They are generally 1-1.3 urn in length, The presence of the microvilli gives them a brush-border appearance.
- Several pinocytic cavities are present within the cell membrane of these microvilli. The microvilli help the lysosome, in protein endocytosis. They serve to increase surface area for reabsorption.
- The upper and lower portions of the cell membrane extend into the cytoplasm as structures, called canaliculi.
- The presence of elongated mitochondria is an important feature of this region. It provides energy for the process of selective reabsorption.
Loop of Henle: The U-shaped portion of the nephron, next to the PCT is called the loop of Henle.
Proximal Convoluted Tubule Characteristics:
- It is about 20 mm in length.
- The loop of Henle (sometimes known as the nephron loop) begins in the cortex, extends into the medulla, and then returns to the cortex.
- Its descending as well as ascending limbs, both have thin and thick regions.
- Like PCT, this region also has elongated mitochondria attached to the basement membrane.
- It has a lesser microvilli
Distal convoluted tubule (DCT): The next convoluted portion of the nephron that arises from the loop of Henle, is called the distal convoluted tubule.
Distal convoluted tubule Characteristics:
- The DCT is about 5 mm long and has an external diameter of 50 mm.
- It is lined by simple cuboidal epithelium, with shorter and fewer microvilli. Hence, there is no distinct brush border.
- A region of this tubule lies very close to the afferent arteriole. This region is called macula densa.
- Macula densa region has tightly packed columnar epithelial cells.
- Cells lining the tubule have mitochondria, attached to the basement membrane. This enables the active transport of ions to take place by the energy supplied by ATP. The plasma membrane has a large number of Canaliculi.
Distal convoluted tubule Collecting duct Definition: The duct that the distal convoluted tubule ends into is called the collecting duct.
Handwritten notes on excretory products and their elimination PDF download
Collecting duct Characteristics:
- The collecting duct is about 20 mm long and pass through both the renal cortex and medulla.
- It is actually not the part of a nephron, rather, the DCTs of several nephrons join together to form one collecting duct.
- Several collecting ducts, carrying urine, join to form the duct of Bellini. This duct enters the renal pelvis.
- The epithelium of the collecting ducts is made up of principal cells (P cells) and intercalated cells (I cells).
- P cells, which predominate, are relatively longer and have few organelles. They are involved in Na+ reabsorption and vasopressin-stimulated water reabsorption.
- I cells, which are lesser in number, have more microvilli, cytoplasmic vesicles, and mitochondria.
- They are concerned with acid secretion and HC03- -transport. Though the collecting duct was previously considered part of a nephron, modern scientists consider it a separate part of the kidney.
Peritubular Capillaries And Vasa Recta
Blood supply in the tubules of nephrons is carried out by peritubular capillaries and vasa recta.
Peritubular capillaries: The network of capillaries, formed by the branching of the afferent arteriole, that runs alongside the nephron and extends over the renal tubule are called peritubular capillaries.
Vasa recta: In the case of juxtamedullary nephrons, peritubular capillaries surround the proximal tubules and distal tubules, as well as Henle’s loop, in a reticulate manner. This is called vasa recta.
Although less than 0.7% of the renal blood enters the vasa recta, these vessels perform many important functions. These include—
Transportation of oxygen and important nutrients to different parts of the nephron.
Delivery of substances to the nephron for secretion.
It serves as a pathway for the reabsorbed water and solutes to enter the circulatory system.
Modification of the concentration of the urine.
Functions Of A Nephron
Nephrons play a very important role in the process of urine formation. Different parts of the nephron perform different functions such as filtration, reabsorption, renal tubular secretion, formation of new substances, etc. These have been discussed in detail in the next section.
Urine Formation Role Of Different Parts Of Nephron
Both nitrogenous and non-nitrogenous wastes are excreted through the urine. Let us study some more about urine and the role of the nephron in urine formation.
Urine Definition: The transparent, yellowish, acidic fluid, with a characteristic pungent odor, that contains nitrogenous and non-nitrogenous excretory products, is called urine.
Urine Characteristics: The following are the characteristics of urine—
Urine Color: Due to the presence of a pigment, called urochrome or urobilin, the urine attains a yellowish color. This color changes in case of different diseases.
Urine Quantity: About 1-1.5 L of urine is produced per day by an adult human being. This quantity may vary with water intake, external environment, physical and mental conditions, etc.
Urine Chemical properties: It is a transparent and acidic fluid. Its pH ranges from 4.5-8.2. Excess intake of animal proteins may increase the acidity, while a diet rich in vegetables, citrus fruits, etc., may decrease the acidity
Odor: Its characteristic odor is that of aromatic compounds. When urine is left for some time, the urea present in the urine gets converted to ammonia, thereby releasing the pungent smell of ammonia.
Constituents of urine
The urine has normal and abnormal constituents. These constituents have been discussed below-
Normal constituents of urine: Urine contains both water and solid constituents. Most of the urine is water (94-96%), with 4-6% of solid constituents.
The solid constituents can be further divided into organic and inorganic constituents. Inorganic constituents are (in 1.5 I L urine volume in 24 hours)— Cl- (6-9 g), NaCI (10-15 g), P043- (0.8-1.3 g), S042- (0.8- 1.4 g), K+ (2.5-3 g), Na+ (4-5 g), Ca2+ (0.1-0.3 g), Mg2+ (0.1-0.2 g), I (50-250 μg), As (50 μg), Pb (50 μg). Organic constituents are further divided into nitrogenous and non-nitrogenous constituents.
Nitrogenous constituents— urea (25-30 g), ammonia (0.7 g), uric acid (0.7 g), hippuric acid (0.1-1.0 g), creatine (60-150 g), creatinine (1.2-1.7 g), amino acid (150-200 mg).
Non-nitrogenous constituents—ketone bodies (0.002-0.012 g), glucose (0.01-0.04 g), oxalic acid (0.014-0.023 g), ascorbic acid (0.014-0.05 g), phenolic compounds (0.2-0.3 g).
Abnormal constituents of urine: These constituents are not found in urine under normal conditions, but are seen in case there is a disease.
These abnormal constituents are discussed as follows—
Glucose: When the glucose concentration in the blood Exceeds 180 mg/100 mL, it results in the release of glucose in the urine. This condition, marked by the presence of glucose in urine, is called glucosuria.
Other carbohydrates: Due to various reasons, fructose, lactose, and galactose may also be released with I urine. These conditions are called fructosuria, lactosuria, and galactosuria, respectively.
The reason behind the more acidic nature of the urine compared to the blood plasma
The glomerular filtrate generated from the blood plasma has an alkaline pH of 7.4, similar to that of blood plasma.
As the filtrate passes through the renal tubule, reabsorption of the sodium ions from the filtrate takes place. Hence, the alkaline nature of the filtrate decreases.
Simultaneously, cells lining the inner walls of the renal tubule secrete hippuric acid, ammonium ion, hydrogen ion, etc., that get mixed with the filtrate. This makes the urine more acidic in nature (pH of 6.0).
Protein: Exhaustive physical work, intake of a high-protein diet, improper metabolism of proteins, inflammation of kidneys, etc., causes the release of excess protein in urine. This condition is known as proteinuria.
Ketone body: The concentration of ketone bodies in the urine increases in case of diabetes mellitus, pregnancy, or improper metabolism of carbohydrates. This condition is known as ketonuria.
Fat: Due to kidney disorder, the poisonous effect of alcohol, etc., excess fat gets released as abnormal constituents of urine. This condition is known as lipuria.
Pigment: Due to a disorder in liver function, bilirubin and biliverdin are excreted through the urine. This condition is mainly found in cases of jaundice or hepatitis.
Blood: Sometimes blood is found in urine, due to internal wounds, inflammation of kidneys, bacterial infection, etc. This condition is known as haematuria.
Alkaptones: The release of excess alkaptones through the urine, occurs in a congenital or hereditary disorder, called alkaptonuria.
Pus: The presence of pus as an abnormal constituent in the urine is seen in the case of some diseases such as urinary tract infections. This condition is called pyuria.
Role Of Different Parts Of The Nephron In Urine Formation
Urine formation in the nephron is the result of successive processes—ultrafiltration, selective reabsorption, and tubular secretion. The different parts of the nephron carry out these processes. Let us study each in detail.
Role of Malpighian corpuscle
The Malpighian corpuscle performs the following functions—
Ultrafiltration: Ultrafiltration is a variety of membrane filtration in which a difference in pressure or concentration across the semipermeable membrane leads to the retention of colloidal particles while smaller particles and the solvent are forced to move across the membrane.
Water, ions, and small nitrogenous molecules from the blood flowing through the glomerulus are filtered into the Bowman’s capsule by this process.
Ultrafiltration Description: The process of ultrafiltration is as follows—
- The visceral layer of the Bowman’s capsule behaves as an ultrafilter. The cells of the Bowman’s capsule and surrounding capillaries form a selectively permeable membrane.
- This membrane allows only water, ions, small nutrient molecules (such as glucose and amino acids), and nitrogenous waste molecules (primarily urea) to pass through it.
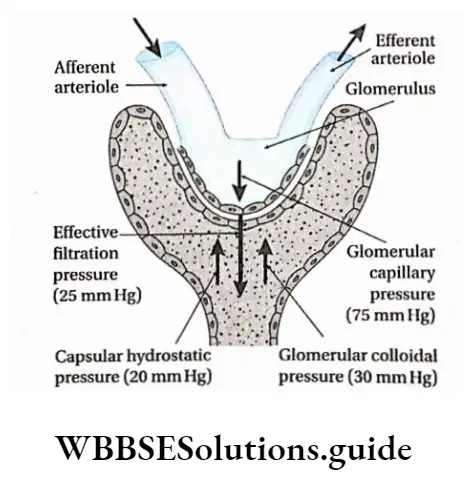
- Blood enters the afferent arteriole and flows into the glomerulus. The high pressure of blood in the glomerulus is called glomerular capillary pressure (GCP). It forces the fluid, containing these molecules and ions, into the capsule.
- Blood cells, platelets, and plasma proteins are too large to pass through. Therefore, they are retained in the capillaries. The charge on molecules as well as their diameters affect their passage into Bowman’s capsule.
- Foot processes have a negatively charged coat (glycocalyx) that limits the filtration of negatively charged molecules, such as albumin. This action is called electrostatic repulsion. All these features of Bowman’s capsule help in the process of filtration of blood.
- The fluid that enters the Bowman’s capsule is an ultrafiltrate of the blood. It is also known as glomerular filtrate or primary urine. The filtrate leaving the Bowman’s capsule is similar to blood plasma in composition, as it passes into the proximal convoluted tubule.
Some factors responsible for ultrafiltration
- The active surface area of the filtration membrane: The active surface area of the filtration membrane depends on the number of active glomeruli and functional blood capillaries present in each glomerulus.
- Permeability of the filtration membrane: Generally, the pores present in the filtration membrane have a diameter of 20-25 nm. Most of the plasma proteins, blood corpuscles, and blood platelets cannot pass through these pores.
However, the colloids present in the blood pressure are called glomerular colloidal osmotic pressure (GOP).
- This pressure along with capsule hydrostatic pressure (CHP) creates a hindrance to ultrafiltration. Both GOP and CHP are known as the opposing pressure. If their total value exceeds Glomerular capsule pressure (GCP) the filtration will occur. The pressure at which the filtration pressure (EFP). The average value of GCP is 75 mm of Hg, while the average values of GOP and CHP are 30 and 20 mm of Hg respectively. The average value of EFP is 25 mm Hg.
- About 1400 L of blood passes through the kidneys every day. The Bowman’s capsule filters about 180 L of fluid from this blood.
- The glomerular filtrate contains wastes such as urea, uric acid, creatinine, excess ions, etc. It also contains glucose, amino acids, etc., some of which get reabsorbed later.
- The amount of glomerular filtrate produced per minute is called the glomerular filtration rate (GFR). The rate of filtration is 125 ml/min. (Jo) Ultrafiltration is driven by Starling forces across the glomerular capillaries. Changes in these forces alter the glomerular filtration rate (GFR). GFR and renal blood flow (RBF) are normally controlled within narrow ranges by a phenomenon called autoregulation.
Storage of ultrafiltrate: The ultrafiltrate is stored in the cavity of Bowman’s capsule for a temporary period.
Role Of Renal Tubule
The glomerular filtrate passes through the renal tubule into the collecting ducts.
The renal tubule carries out three functions—
- Selective reabsorption,
- Tubular secretion,
- Synthesis of some substances.
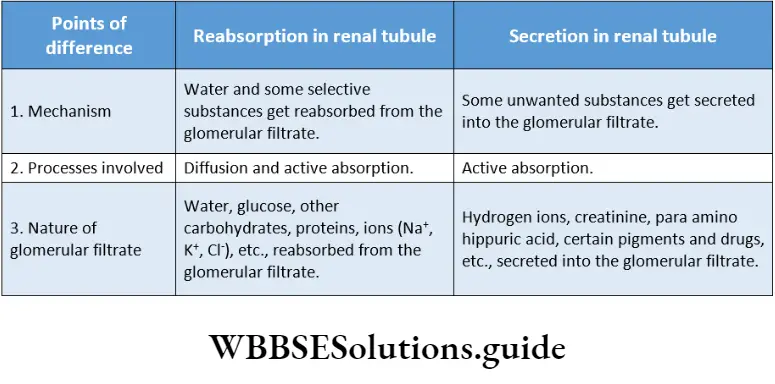
Selective reabsorption: The reabsorption of filtered molecules, such as H+, Na+, and K+ ions from the glomerular filtrate in the tubules to the blood is called selective reabsorption.
About 85% of the 180 L of glomerular filtrate, formed per day, is reabsorbed by this process.
This reabsorption, as well as the regulated reabsorption of the remaining volume of filtrate, occurs by osmosis. It results in the transport of Na+ and Cl– ions across the tubule wall.
A concentration gradient is created between tubular filtrate and the plasma, in the surrounding capillaries. This promotes the osmosis of water back into the vascular system.
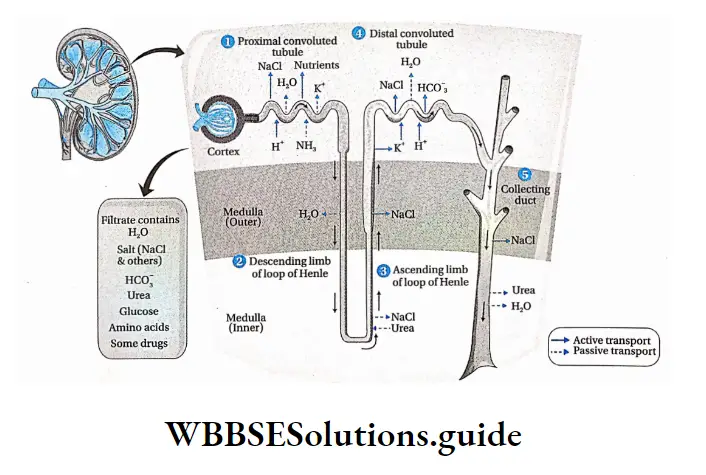
Reabsorption in proximal convoluted tubule: The proximal convoluted tubule reabsorbs approximately 67% of the filtered water, Na+, K+, CP, and other solutes.
In addition, the PCT also reabsorbs most of the glucose and amino acids filtered by the glomerulus.
The key element, in proximal tubule reabsorption, is the Na+K+ATPase, which is found in the basolateral membrane. The reabsorption of every substance, including water, is linked in some way to the operation of this enzyme.
Specialized ion pumps transport K+, Na+, and C– from the filtrate into the fluid surrounding the tubule.
Active transport proteins, embedded in the walls of the tubule, reabsorb the amino acids, glucose, and other nutrients out of the filtrate.
Water, chloride ions, and urea are absorbed passively, whereas substances like hormones, amino acids, sulfates, phosphates, etc., are absorbed through active transport.
The coiled structure and microvilli greatly increase the total surface area that is available for the reabsorption of solutes.
The reabsorption of solutes makes the filtrate hypoosmotic to the interstitial fluid. This causes water to flow out of the tubule, into the interstitial fluid by osmosis.
The reabsorption of water in PCT is obligatory in nature. The movement of water is further facilitated by membrane proteins, called aquaporins.
The aquaporins ensure that the maximum water is removed from the tubule during the reabsorption process. The presence of a large number of mitochondria provides the energy to carry out the process of reabsorption.
Reabsorption in a loop of Henle: The fluid, which has a high concentration of urea and other unabsorbed wastes, moves through the proximal convoluted tubule into the descending portion of the loop of Henle.
The descending limb of the loop of Henle is permeable to water, due to the presence of aquaporin-1, in both the apical and basolateral membrane. About 15% of the filtered water is removed from the descending limb.
Therefore, the fluid in the descending limb of the loop of Henle becomes hypertonic, to plasma.
However, the ascending limb is impermeable to water. Na+, K+, and Cl– are co-transported out of the thick segment of the ascending limb.
Bivalent ions like Mg2+, Ca2+, etc., are also reabsorbed actively in this region. This dilutes the solution. In the ascending limb, it becomes more dilute because of the movement of Na+ and Cl– out of the tubular lumen.
Thus, the fluid becomes hypotonic to plasma, when it reaches the top of the ascending limb Hence, this portion of the nephron is called the diluting segment.
Reabsorption in distal convoluted tubule: The distal tubule is relatively impermeable to water. So, water reabsorption is facultative here.
The reabsorption of water is regulated by ADH or antidiuretic hormone (vasopressin). Due to sweating, continued removal of the solute further dilutes the tubular fluid.
Under such conditions, ADH is secreted. It stimulates the cells of the DCT and the collecting duct, which are otherwise impermeable to water, to reabsorb water.
After passing through the distal convoluted tubule, only 3% of water remains in the filtrate.
The salt content remaining in the filtrate is negligible. About 97.9% of the water in the glomerular filtrate gets absorbed in the PCT, loop of Henle and DCT.
Obligatory Water Loss
Although about 180 L of glomerular ultrafiltrate is produced every day, the kidneys normally excrete only 1 to 2 L of urine in a 24-hour period.
The urine volume, however, varies according to the needs of the body.
When a well-hydrated person drinks more water, urine production increases to 16 ml per minute. If this situation continues, 23 L of urine may be excreted per day.
On the other hand, in case of severe dehydration, when the body needs to conserve water, only 0.3 ml of urine per minute, or 400 ml per day, is produced.
A volume of 400 ml of urine per day is the minimum needed to excrete the metabolic wastes produced by the body; this is called obligatory water loss.
Tubular secretion: The secretion of certain substances, such as H+, urea, etc., into the glomerular fluid, when it passes through the DCT is called tubular secretion.
Tubular secretion leads to the removal of waste products from the blood and interstitial fluid.
These waste products are hydrogen ions, creatinine, para amino hippuric acid, certain pigments, and drugs.
H+ ions are actively secreted, while the products of detoxified toxins, produced by the liver, are passively secreted. Many water-soluble drugs, such as penicillin and other medications, along with their metabolites are also secreted into the nephron.
Some amount of ammonia is also secreted into the tubule. H+ secretion is coupled with HCO– reabsorption from the filtrate to the plasma in the peritubular capillaries. The release of certain hormones triggers changes in the salt concentration in the body.
This varies the secretion of K+ and H+ ions into the filtrate in the DCT. Additionally, active secretion of H+ occurs in the collecting ducts. The balance of ions established in the blood, urine, and interstitial fluid, regulates the pH level of the blood and body fluids.
In this way, the kidney acts as a “safety valve.” If the acidity of the body fluid rises, the excess H+ ions are secreted into the collecting ducts. These ions are then excreted through the urine.
New product formation: Different substances like ammonia, hippuric acid, etc., are synthesized by the cells, lining the renal tubule. These substances are released into the lumen of the tubule and pass out of the body a,ong with the urine.
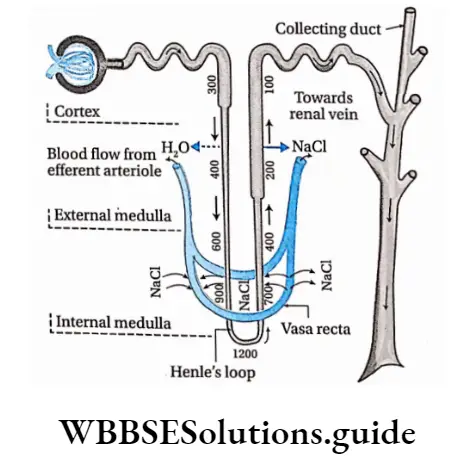
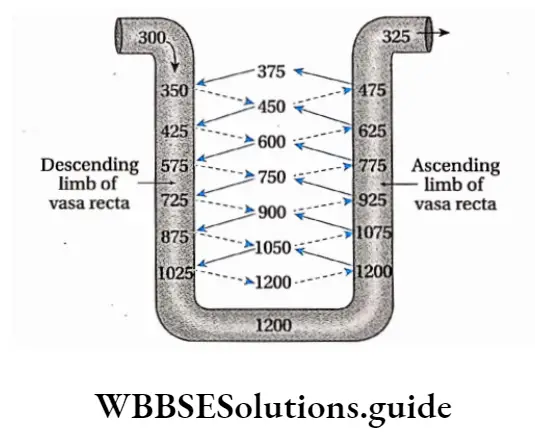
Mechanism For Concentration Of Glomerular Flarte The Countercurrent Mechanism
Mechanism For Concentration Of Glomerular Flarte Definition: The mechanism, present within the nephron that regulates the balance of water, ions, and pH within the blood and interstitial fluid, is called the countercurrent mechanism.
The loop of Henle and vasa recta play important roles in the countercurrent mechanism. In this mechanism, the interplay occurs between the isotonic tubular fluid and the blood flowing in the opposite direction through the vasa recta. The name ‘countercurrent’ indicates the opposite direction of flow of the two fluids.
Mechanism For Concentration Of Glomerular Flarte Types: This system involves two separate types of subsystems.
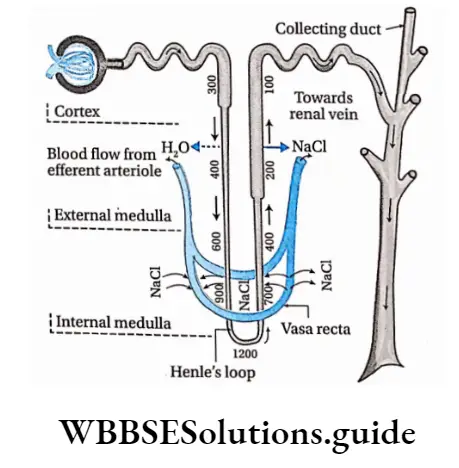
Countercurrent multiplier: The gradient of increasing osmolarity produced by the activity of the loop of Henle, in the renal medulla, acts as a countercurrent multiplier. This makes the interstitial fluid in the renal medulla, hypertonic.
Countercurrent exchanger: In this system, the hypertonicity of the interstitial fluid is maintained in the renal medulla, by exchanging ions between the blood and the tubular fluid. The Vasa Recta Along The loop of henle acts as a countercurrent exchanger.
Significance of countercurrent mechanism:
Due to the Countercurrent mechanism, the nephrons are able to produce hyper or hypotonic urine. This maintains the osmolarity of the body fluids and blood.
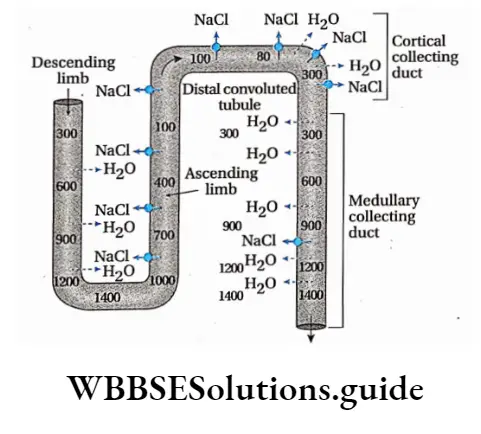
Countercurrent multiplier mechanism in the loop of Henle:
- It is an energy-driven process that generates an osmotic gradient along certain sections of the renal tubule (Henle’s Loop and DCT, collecting duct).
- The loop of Henle is bathed in hypertonic interstitial fluid in the medulla. Its descending limb is permeable to water.
- Thus, water moves out of the tubular fluid making it concentrated. This water readily enters the vasa recta and is carried away. This rapid removal of water from interstitial fluid maintains its hypertonicity.
- As the fluid gradually moves through the descending limb, more water gets reabsorbed, but, urea and other ions such as Na+, and K+ do not get reabsorbed. This increases the osmotic concentration of tubular fluid up to 1200 mOsmol L-1.
- This hypertonic filtrate moves up to the ascending limb of Henle’s loop. Here water does not get reabsorbed as its wall is impermeable to it. But, a large amount of Na+ and Cl” is reabsorbed via active transport. Hence, the filtrate becomes isotonic (with respect to blood).
- Consequently, tubular fluid rises through the ascending limb, along with active reabsorption of NaCI, while, urea passively diffuses into the tubular fluid. The osmotic concentration of the filtrate lowers to about 100 mOsmol L-1.
- Some reabsorption takes place in the DCT due to the action of ADH hormone, this increases the osmotic concentration of the filtrate to about 300 mOsmol L-1.It depends on
- The high permeability of the thin descending limb to water (via aquaporin-1),
- Active transport of na+ and clout of the thick ascending limb, and
- Inflow of tubular fluid from the PCT, and its outflow through the DCT.
Countercurrent Exchanger Mechanism in the vasa recta:
- Blood enters and leaves the medulla through the vasa recta present at the boundary of the cortex and the medulla. These capillaries are highly permeable to solute and water.
- As the blood descends into the medulla towards the papillae via the descending limb of the vasa recta, it becomes more concentrated by gaining solutes and losing water to the hypertonic interstitial fluid.
- By the time blood reaches the tip of the ascending limb of the vasa recta, it has an osmotic concentration of 1200 mOsmol L-1.
- As this hypertonic blood moves towards the ascending limb of the vasa recta (towards the cortex) solutes diffuse back into the interstitial fluid and the water diffuses back into the blood, making it isotonic.
- Under normal conditions, vasa recta carries away only as much solute and water as is absorbed from the tubules. In this way, the high concentration of solutes is established in the interstitial fluid and the countercurrent mechanism is maintained.
- The ability of the vasa recta to maintain the osmotic gradient of interstitial fluid in the medullary region is flow-dependent.
- A substantial increase in blood flow through the vasa recta will ultimately disrupt the medullary osmotic gradient.
- Alternatively, if blood flow is reduced, the nephron segments within the medulla will receive inadequate oxygen.
- This will disrupt the active transport of ions across the ascending limb of Henle’s loop. As a result, the medullary osmotic gradient will be disrupted.
Osmotic concentration
The osmotic concentration of a solution is the concentration of particles that remain dissolved in that solution. It is generally expressed as milli osmoles 1 per liter (mOsmol L-1).
Osmorecepter
There are certain receptors in the body that can sense the change in the osmolarity of the body fluids. These receptors are called osmoreceptors. These are located in the anterior hypothalamus in the brain.
They respond only to certain solutes that are called effective osmoles. Certain solutes such as urea, do not affect the function of the osmoreceptors; These are called ineffective osmoles.
NEET excretory products and their elimination revision notes with MCQs
Role of countercurrent mechanism in producing hypertonic urine:
- As the tubular fluid passes through the descending limb of the loop of Henle, more water gets reabsorbed into the blood. But Na+ and other ions do not get reabsorbed, hence the osmolarity of the tubular fluid increases.
- As the tubular fluid passes through the ascending limb, some of the Na+ ions get reabsorbed, lowering the osmolarity of the tubular fluid.
- Finally, when the tubular fluid passes through the DCT, hormones like ADH and aldosterone, cause some more of the Na+ ions to be reabsorbed in the renal medulla. This increases the osmolarity of the tubular fluid again.
- Some amount of water also gets reabsorbed when the tubular fluid passes deeper into the renal medulla. Along with this, some amount of urea diffuses into the tubular fluid from interstitial fluid by passive transport.
- This leads to the release of hypertonic or hyperosmotic urine (1200 mOsmol L-1). Hypertonicity of urine is measured against blood and plasma.
Micturition
Micturition Definition: The biological process by which the urine stored in the urinary bladder gets excreted by the urethral orifice to the exterior, is called micturition.
Process: Micturition is initiated through the coordinated contraction of certain muscles. These are smooth muscles present within the walls of the urinary bladder, thoracic and pelvic region, diaphragm, and internal and external sphincter muscles.
The process may be described as follows—
- The urine produced within the nephron is carried by the ureters to the urinary bladder, where it is stored temporarily.
- The urine storage capacity of the urinary bladder in humans is about 800 ml.
- However, stretch receptors (nerve endings under the control of the autonomic nervous system), present within the walls of the urinary bladder, get stimulated when
about 300-400 ml of urine gets stored within it. - When the amount of urine in the urinary bladder increases further, this stimulus is carried to the brain and this generates the urge to urinate.
- The detrusor muscles, present within the walls of the urinary bladder, contract under the influence of efferent autonomic nerves.
- At the same time, sphincter muscles associated with the urethra, relax. As a result, the urine passes through the urethra and gets excreted out of the body through the urethral orifice.
- It is to be noted that contraction of the diaphragm and the muscles of the thoracic region, help in micturition. In the case of infants, some elderly adults, and those with neurological injuries, micturition is an involuntary reflex action.
Osmoregulation
Osmoregulation Definition: The regulatory mechanism, by which the living organisms maintain the balance of water and different ions within the cells as well as body fluids (blood, lymph, etc.), is called osmoregulation.
Osmoregulation Discussion: Water and ions are lost by various metabolic processes.
- Even the external environmental factors lead to the imbalance of water and ions. Water loss through sweat, feces, and during respiration from the lungs cannot be regulated.
- In contrast, renal excretion of water is regulated to maintain water balance in the body.
- Our body has well-developed mechanisms to maintain the osmotic concentration- of the body fluids.
- The water intake must precisely match the water loss from the body. When water intake is low or water loss is high, the kidneys conserve water by producing less urine.
- The urine becomes hyperosmotic with respect to plasma. When water intake is high, a large volume of hypoosmotic urine is produced.
- In a normal individual, the osmolarity of urine may vary from approximately 50 to 1200 mOsmL-1 of water. The corresponding urine volume may vary from as much as 18 L/day to as little as 0.5 L/day.
Significance: The significance of osmoregulation is—
Maintenance of osmotic concentration of body fluids: The osmotic concentration of the body fluids such as blood, lymph, etc., can be maintained by osmoregulation. If intake of water exceeds loss of water, then the water balance is positive. Conversely, when the intake of water is less than the loss of water, then the water balance is negative.
Maintenance of Homeostasis: It is maintained in extracellular fluids, by osmoregulation.
Rate of metabolic reactions: The rate of metabolic reactions is maintained properly within the cells by osmoregulation.
Excretory Class 11 Notes
Regulation Of Kidney Function
Neural signals, hormonal signals, and intrarenal chemical messengers combine to regulate the renal processes according to the needs of the body.
Neural signals: They originate in the celiac plexus of the sympathetic nervous system. These signals exert major control over renal blood flow and glomerular filtration.
They also influence the release of vasoactive (affecting blood vessels) substances, like angiotensin, that affect both the kidneys and the peripheral blood vessels.
Hormonal signals: They originate in the adrenal gland, pituitary gland, heart, and kidney itself. Their effects are as follows—
The juxtaglomerular apparatus of the kidney secretes renin and affects the GFR and blood pressure.
The posterior pituitary gland secretes the hormone vasopressin (also called antidiuretic hormone or ADH).
ADH is a major regulator of excretion. Through its influence on the renal blood vessels and principal cells of the collecting duct, it probably affects sodium excretion as well.
The heart muscles secrete hormones such as atrial natriuretic peptides (ANP), a vasodilator that increases sodium excretion by the kidneys. Hormones like aldosterone, secreted by the adrenal cortex, also influence the sodium and potassium ion balance.
Intrarenal chemical messengers: They also show some effect on the process of urine formation.
It is clear that an array of substances (e.g., nitric oxide, purinergic agonists, superoxide, etc.) influence basic renal processes, but, for the most part, the specific roles of these substances are not well understood.
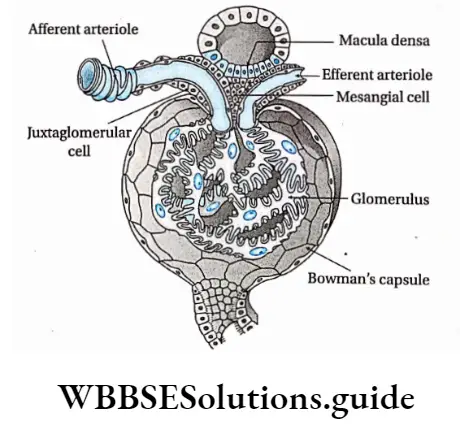
Juxtaglomerular Apparatus
Juxtaglomerular Apparatus Definition: The organization of certain types of cells, present near the region, where the DCT lies close to the afferent arteriole, and responsible for renin secretion is called juxtaglomerular apparatus (JGA).
Structure: Each JGA is made up of the following three cell types—
Granular cells: Granular cells juxtaglomerular cells), are the smooth muscle cells, present in the walls of the afferent arterioles.
The granular cells are so named because they contain secretory vesicles that appear granular under a light microscope. These granules contain the hormone renin.
Extraglomerular mesangial cells: Extraglomerular mesangial cells are morphologically similar and continuous with the glomerular mesangial cells, but lie outside Bowman’s capsule.
They lie in the region extending between the afferent and efferent arteriole. These cells are also known as lacis cells.
Macula densa cells: These are specialized thick epithelial cells. They are present in the region where the DCT lies close to the afferent arteriole.
These cells can detect the composition of the fluid within the nephron at the extreme end of the thick ascending limb of the loop of Henle. They help to control renin secretion.
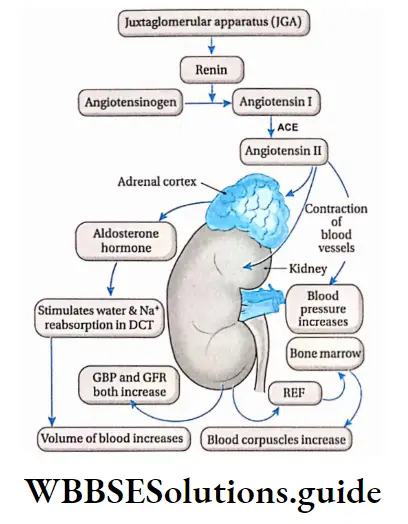
Juxtaglomerular Apparatus Functions:
When the blood pressure falls due to reduced blood flow to the kidneys, the sympathetic nervous system generates a stimulus. This stimulus causes the JGA to secrete renin.
It generates a decapeptide angiotensin-l by splitting angiotensinogen, a plasma protein. This under the influence of angiotensin-converting enzyme (ACE), forms angiotensin 2. This, in turn, stimulates the secretion of aldosterone from the adrenal cortex.
Aldosterone increases the reabsorption of water and Na+ ions in the DCT, thereby increasing the blood flow which raises the blood pressure. It finally increases the glomerular filtration rate (GFR).
During the shortage of oxygen in tissues, JG cells secrete a hormone called erythropoietin or renal erythropoietic factor (REF). This stimulates the production of RBCs in the bone marrow.
Atrial natriuretic peptide (ANP)
Atrial natriuretic peptide (ANP) Definition: The proteinaceous substance, secreted by the atrium of the heart, that acts as a vasodilator and maintains the balance between water and sodium ions in blood, is called an atrial natriuretic peptide (ANP)
Atrial natriuretic peptide Description: Earlier, it was considered that there are some factors that regulate the excretion of Na+ through urine. The process was termed natriuresis and the factors were called natriuretic factors.
Later, it was discovered, that cardiac atria secrete a factor with such a function. The first natriuretic hormone isolated from the heart was atrial natriuretic peptide (ANP).
The hormone ANP is also known as atrial natriuretic factor (ANF). ANP was subsequently isolated from other tissues, including the brain, where it exists in two forms that are smaller than circulating ANP.
Its secretion is stimulated by a rise in blood pressure and an increase in the effective i circulating volume.
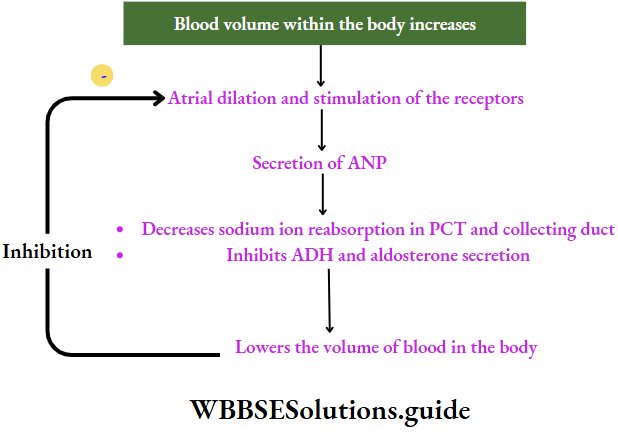
Functions: It has effects both on the kidney and the blood pressure. The effects are as follows—
On kidneys:
- It inhibits NaCI reabsorption by the medullary portion of the collecting duct.
- It inhibits ADH- ADH-stimulated water reabsorption across the collecting
duct.
On blood pressure:
It reduces blood pressure by dilating the walls of the heart and enhancing urinary NaCI and water excretion.
It inhibits the secretion of renin by the JGA which in turn inhibits the secretion of aldosterone by the adrenal cortex. This promotes the excretion of sodium along with water. This causes blood pressure and blood volume to decrease.
It reduces the secretion of ADH from posterior pituitary.
ANP secretion by the heart rises with hypertension and expansion of extracellular fluid volume, causing vasodilation of the afferent arteriole and vasoconstriction of the efferent arteriole.
The net effect of ANP is therefore to produce a mild increase in GFR with little change in RBF (renal blood flow).
Disorders due to sodium imbalance in the blood
Hypernatremia: If the sodium level in blood plasma is above normal (130-145 mmol/L), the condition is called hypernatremia.
Hyponatremia: If the sodium level in blood plasma is below normal, the condition is called hyponatremia.
Human excretory system: structure, function, and waste elimination process
Antidiuretic Hormone (ADH) And Diabetes Insipidus
The hormone, secreted by the pituitary gland, that acts on the kidneys to regulate the volume and osmolarity of the urine, is called antidiuretic hormone (ADH) or vasopressin.
Source of ADH: It is synthesized by neuroendocrine cells within the hypothalamus region of the brain. The synthesized hormone is packed in granules. These granules are stored at the nerve terminals in the posterior pituitary.
Functions of ADH:
- ADH increases the reabsorption of water in the DCT and the collecting duct.
- When plasma ADH levels are elevated, less volume of concentrated urine is excreted. This condition is called antidiuresis.
- When plasma ADH levels are low, more volume of urine is excreted. This condition is called diuresis. The urine, that is released, is dilute.
- It lowers the reabsorption of Cl” ions and thus large quantities of CP ions are excreted through the urine.

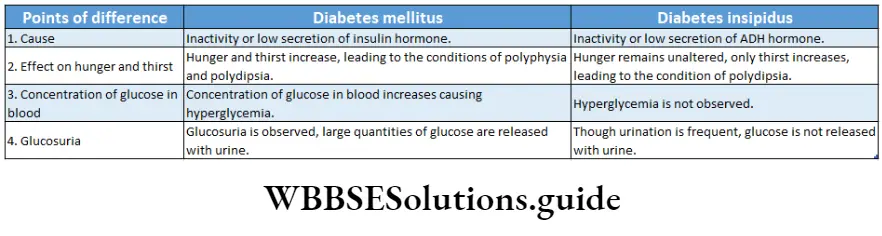
Diabetes insipidus Definition: The syndrome, that is characterized by the release of a large volume of hypotonic urine due to deficiency of ADH hormone in the blood or due to malfunctioning of kidneys, is called diabetes insipidus.
Causes: The causes of diabetes insipidus are—
Damage or infection of pituitary gland or associated neurons: If certain regions of the nervous system (the supraoptic and paraventricular nuclei, the hypothalamohypophysial tract), or the posterior pituitary gland gets damaged or infected, diabetes insipidus results.
The disease may develop after surgical removal of the posterior lobe of the pituitary. However, this condition may be temporary. The fibers may recover, make new vascular connections, and begin to secrete vasopressin again.
Failure of ADH to bind to receptors: If the ADH cannot bind to V-2 receptors (a type of vasopressin receptor) due to kidney malfunctioning, this disease may result. It mainly occurs as a genetic defect.
Mutation of water channel proteins aquaporin-2: It inhibits the reabsorption of water in the DCT and collecting duct. This situation may also develop this disease.
Types: Diabetes insipidus is generally of the following two types—
Vasopressin-sensitive or neurogenic or central diabetes insipidus: The type of diabetes insipidus caused by the damage of the hypothalamus or posterior pituitary gland, leading to less ADH secretion is called vasopressinsensitive or neurogenic or central diabetes insipidus.
Low vasopressin secretion decreases water and salt reabsorption in the DCT and collecting duct. This leads to the frequent discharge of dilute urine.
Nephrogenic diabetes insipidus: The type of diabetes insipidus that occurs due to malfunctioning of the kidneys, is called nephrogenic diabetes insipidus. Two forms of nephrogenic diabetes insipidus are generally seen.
In one form, the gene for the type 2 vasopressin receptor (V2) is mutated, making it unresponsive.
In the other case, mutations occur in the autosomal gene for aquaporin-2. This in turn, gives rise to mutated aquaporin-2 proteins.
These mutated aquaporins get trapped in intracellular locations, instead of reaching the collecting duct. This impairs the reabsorption of water and leads to frequent urination, releasing more volumes of urine.
Nephrogenic diabetes insipidus Symptoms:
- This disorder is marked by frequent urination. This condition is called diuresis.
- The symptoms of diabetes insipidus include the passing of large amounts of dilute urine. This condition is called polyuria.
- ADH stimulates thirst. Increased ADH secretion generates excessive thirst which leads to the intake of large quantities of water, which may lead to a medical condition called polydipsia. But, this is what keeps these patients healthy.
- If their sense of thirst is depressed for any reason and their intake of dilute fluid decreases, they develop dehydration that may be fatal.
- Excessive thirst causes dryness of the mouth.
Nephrogenic diabetes insipidus Treatment: Desamino D-Arginine Vasopressin (DDAVP) is a medication prescribed for this disorder. It has similar functions as ADH.
Role Of Other Organs In Ecreation
Besides the kidneys, there are certain other organs that remove waste products from the body. These include liver, skin, lungs, etc.
Role Of Skin
Skin is the largest organ in the human body. It is an accessory excretory organ. The skin contains sweat glands and sebaceous glands. The sweat glands secrete sweat while the sebaceous glands secrete sebum.
The different excretory functions of the skin have been discussed below.
Sweating:
There are numerous sweat glands present in the skin. They are microscopic, tubular structures that remain coiled within the dermis.
They are surrounded by a network of blood capillaries. They open up on the skin through minute pores.
These glands absorb several metabolic wastes such as urea, salts, and amino acids along with excess water from the blood and excrete them through the sweat.
The sweat glands remain very close to the blood capillaries. Thus, the metabolic wastes can diffuse out of the blood and enter the sweat glands. From here, these are excreted through the sweat.
In addition to excreting metabolic wastes, sweat also provides a cooling effect to the body.
About 1-1.5 L of sweat is excreted per day.
Types of sweating: Sweating is of two types.
Sensible sweating or perspiration: Sensible sweating or perspiration is a form of sweating or perspiration that can be sensed by the body. This perspiration absorbs the latent heat of the body, providing a cooling effect.
Insensible sweating or perspiration: Insensible sweating or perspiration is a kind of sweating or perspiration that occurs before the body can sense it. This can happen through the skin, mucous membranes of the lungs, and nasal cavity, in the form of vapor only. It is an obligatory process and has no connection with the sweat glands.
Other roles: A small amount of carbon dioxide gets excreted through the skin. It is about 1/100th of that excreted through the lungs. The skin of the external auditory meatus, in the external ear, contains ceruminous glands. They secrete a wax-like substance called cerumen. It contains several waste products.
Sebum, secreted by sebaceous glands, is an oily fluid. Different types of, sterols, fatty acids, etc., are excreted through the sebum.
Role Of Lungs
The lungs act as an accessory excretory organ besides being the principal respiratory organ.
The functions of; the lungs as excretory organs are as follows—
- About 18 L of C02 is produced every day by respiration. This is eliminated from our body through the air expired by the lungs.
- About 400 ml of water vapor is released from the body to the environment per day, through the expired air.
- Small amounts of acetone, ammonia, alcohol, etc., get excreted from the body by the lungs.
Role Of Liver
The liver is responsible for detoxifying and breaking down any toxin that enters our bodies.
Ammonia gas is generated within the body by deamination reactions. It is harmful to the body. The liver converts ammonia into urea, by the ornithine cycle. The liver filters the blood and recycles older and damaged RBCs.
It removes the following substances through the bile—heavy metals like copper, zinc, etc., certain drugs, bacteria, toxins from the blood (like alcohol), bile pigments and cholesterol, lecithin, etc.
Role Of Salivary Glands
The salivary gland produces saliva, which contains certain waste products, for example, inorganic salts, organic substances like urea), some drugs, and heavy metals such as lead, mercury, etc People who consume alcohol, excrete it through saliva. Large amounts of thiocyanates are present in the saliva of smokers. Even the microbes causing several diseases get released through the saliva.
Role Of Large Intestine
The feces, which are formed in the large intestine and eliminated from the body through the anus, contain heavy metals (e.g., bismuth, mercury, etc.), bile pigments, drugs, and many more waste products. Therefore, the large intestine also serves as an accessory excretory organ.
Disorders Related To Excretory System
Some of the different disorders related to the excretory System-
Uremia Definition: The disorder caused due to profound renal malfunction, that leads to the accumulation of urea and other nitrogenous wastes in the blood instead of being excreted with the urine is called uremia.
Excretory System Causes:
- It develops if urea concentrates in the blood instead of getting released through the urine due to renal malfunction.
- It develops when the byproducts of protein metabolism other than urea, such as creatinine, amino acids, etc., accumulate in the blood.
Excretory System Symptoms:
- Anorexia, Symptoms of vomiting, and uremia include mental deterioration, confusion, muscle twitching, convulsions, and coma.
- The blood urea nitrogen (BUN) and creatinine levels are high. The blood levels of these substances are used as an index of the severity of uremia.
- It includes the accumulation of urea and creatinine along with that of other toxic substances (organic acids or phenols)
Excretory System Treatment:
- Patients or the ones vulnerable to uremia are often haemodialysed by using a dialysis machine. This procedure has been described later in detail.
- Another method to treat uremia is haemofiltration. It involves filtering the blood under high pressure.
Renal failure
Renal failure Definition: The malfunctioning of the kidneys either acute or chronic, caused due to low glomerular filtration rate (GFR) resulting in the accumulation of nitrogenous substances in the blood, is called renal failure.
Renal failure Causes: Renal Failure may occur due to
- Bacterial infection
- Injuries
- Hemorrhage in the kidneys
- A disease called glomerulonephritis (inflammation of glomeruli),
- less electrolyte concentration in the body fluids.
Renal failure Types: It is generally of the two types—
Acute renal failure (ARF) —in this case, the kidneys lose their ability to excrete wastes and to regulate the homeostasis of blood volume, pH, and electrolytes. It deteriorates over a relatively short period of time (hours to days).
Chronic renal failure—it is the slow deterioration of the renal functions, that extend for a much longer period and finally lead to symptoms of uremia.
Symptoms: It results in failure to excrete different waste products from the body. Its symptoms include uremia, accumulation of wastes in the blood, disruption of water-salt balance in the body, and failure to secrete erythropoietin.
Renal failure Treatment:
- Avoiding medications that may cause renal failure as a side-effect.
- Haemodialysis may also be prescribed.
Nephritis
Nephritis Definition: Inflammation of the kidneys is called nephritis.
Nephritis Causes: It can be caused by infection, but is most commonly caused by autoimmune disorders that affect the major organiser
Nephritis Types: It may involve inflammation of the glomeruli, renal tubules, or interstitial tissue surrounding the glomeruli and tubules.
It is generally of two types—
- Glomerulonephritis and
- Pyelonephritis.
Nephritis Symptoms:
Symptoms of glomerulonephritis include proteinuria and haematuria.
Nephritis causes additional problems like water retention, as the kidneys cannot function properly to excrete water. Water retention or edema, can further cause swelling of the feet, ankles, legs, and hands.
In the case of pyelonephritis, the concentration of the urine decreases, leading to painful urination and severe body ache.
Nephritis Treatment: Primarily, nephritis tends to be treated with antibiotics. Occasionally it is treated with steroids, particularly in those cases when it is caused by lupus (an immune system disease). However personal hygiene is important as microbial contamination is one of the major causes of this disease.
Differences between ammonia, urea, and uric acid excretion
Renal Calculi
Renal Calculi Definition: The solid aggregations of the minerals in the urine, that do not get excreted, are called kidney stones or renal calculi.
Renal stone calculus or lithiasis is one of the most common diseases of the urinary tract. It occurs more frequently in men than in women. It is rare in children.
It shows a familial predisposition. Urinary calculus is a stone-like body, composed of urinary salts bound together by a colloid matrix of organic materials.
Renal Calculi Causes: The causes of renal calculi are—
Renal Calculi Dehydration: Due to dehydration, water reabsorption increases but reabsorption of the ions does not take place. This leads to their accumulation as calculi.
Changes in pH of the urine: If the buffering system in the kidneys gets affected, the urine that is released becomes alkaline. Substances like phosphates, etc., that form calculi, are released with such urine.
Microbial contamination: When crystalline substances form layers over pus, tissue fragments, etc., produced by microbial contamination, kidney stones are formed.
Metabolic conditions: Hyperparathyroidism, gout, etc., are also other causes of the formation of kidney stones.
Accumulation of calcium, uric acid, and oxalates leads to the formation of kidney stones.
Renal Calculi Types: Basically the renal stones can be divided into two major groups—
Primary stones: They appear in apparently healthy urinary tract without any preceding inflammation.
Secondary stones: They are usually formed as a result of inflammation.
Renal Calculi Symptoms: The symptoms include pain in the pelvic area and lower abdomen. This condition is called renal colic. It is associated with haematuria and painful urination. If the kidney stones descend and block the urethra, it may prevent the passing of urine through it. Retention of urine inside the bladder may result in urinary tract infection.
Renal Calculi Treatment: The kidney stones may be removed by surgery. Nowadays, laparoscopy is used to remove kidney stones.
In this process, the stones are collected from the kidney or the ureter through a small incision made in the respective organ. It is also called ‘keyhole surgery’.
The use of medicines like allopurinol (decrease uric acid production), diuretics, etc., may prevent the formation of stones in the kidney.
Another measure for treatment of the kidney stones is lithotripsy. It involves mechanical destruction of the kidney stones. Fragments of the stones are excreted through the urine.
Some other renal disorders body towards the dialyzer
Glomerulonephritis: This involves inflammation of the glomerulus.
Pyelonephritis: This involves inflammation of the renal pelvis due to infection in the ureters.
Some Important Procedures For Treatment Of Renal Disorders
There are some treatment procedures that are important for treating the above disorders. Some of them are discussed below.
Dialysis And Artificial Kidney
Dialysis and artificial kidney Definition: The clinical procedure by which the blood is purified artificially is called dialysis.
Dialysis uses the principle of diffusion of molecules, from high to low concentration.
In this process the diffusion occurs through a natural or synthetic semipermeable membrane, that allows only small molecules to pass through. This membrane is called a dialysis membrane. Dialysis is generally of two types.
Haemodialysis
The term dialysis refers to the separation of molecules on the basis of their ability to diffuse through an artificially selectively permeable membrane.
The principle of ultrafiltration is used in the “artificial kidney machine”, which is generally used for hemodialysis. This machine is also called the dialysis machine.
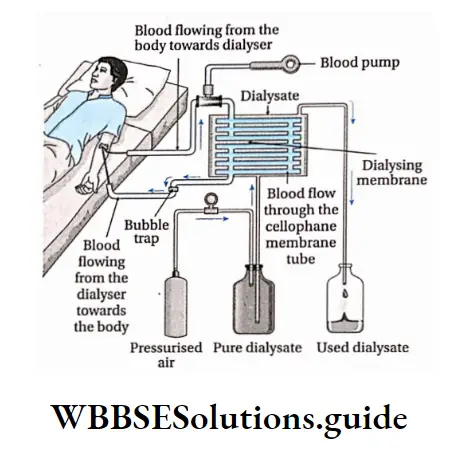
Haemodialysis Process:
In a dialysis machine, the patient’s blood with heparin at 0° C flows slowly through many small channels made of semipermeable membranes, through which only small molecules can diffuse.
A dialyzing solution or dialysate flows on the other side of these membranes.
The composition of this dialysis solution is crucial. It contains water, glucose, and electrolytes like sodium, potassium, calcium, magnesium, and chloride. This composition varies with the patient’s needs.
The total osmotic potential of the dialysis fluid must be equal to that of the plasma.
Molecules such as urea, uric acid, creatinine, etc., and ions that need to be removed from the blood are absent in the dialysis fluid.
These molecules and ions diffuse from the area of higher concentration (patient’s blood) to the area of lower concentration (dialyzing fluid). Thus, the blood in the patient’s body is purified by the removal of harmful products.
About 500 ml of the patient’s blood is in the dialysis machine at any one time, and the unit processes several hundred milliliters of blood per minute.
A patient with severe renal failure must be on the dialysis machine for 4 to 6 hours, three times a week.
Importance of hemodialysis: Loss of kidney function or renal failure, results in uremia.
A person who suffers complete renal failure may die within 2 weeks, if not treated.
A drastic but highly successful treatment for such patients is a kidney transplant, but it needs a donor with proper compatibility with the patient. Therefore, artificial kidneys may be used as an immediate option.
Peritoneal dialysis
When the peritoneum inside the person’s body is used as the dialysing membrane, it is known as peritoneal dialysis.
Kidney Transplantation
Hemodialysis is not the permanent solution to complete renal failure. The damaged kidneys need to be transplanted by healthy kidneys from donors. This procedure is called kidney transplantation.
Excretory Products And Their Elimination Notes
- Catabolism: A series of metabolic reactions which break down complex molecules into simpler units.
- Chemical messengers: Metabolites that transport messages from one part of the body to the other, e.g., hormones, neurotransmitters, etc.
- Endocytosis: This is a form of active transport in which a cell engulfs foreign particles.
- Hemorrhage: Escape of blood from a ruptured blood vessel.
- Homeostasis: The tendency towards a relatively stable equilibrium between interdependent elements, especially as maintained by physiological processes.
- Peritoneum: The membrane that forms the lining of the abdominal cavity or coelom.
Points To Remember
- The organ system, that is responsible for the release of waste products from the body, is called the excretory system.
- Wastes generated from the body may be nitrogenous (urea, ammonia, uric acid, etc.) and non-nitrogenous (C02, oxalic acid, etc.).
- Organisms can be ammonotelic, ureotelic or uricotelic. Human beings are ureotelic.
- Protonephridia, metanephridia, and malpighian tubules are excretory organs found in different invertebrate organisms.
- The human excretory system consists of a pair of kidneys, a pair of ureters, a urinary bladder, and a urethra.
- According to the structure, the kidney can be pronephric (primitive structure), mesonephric (slightly modified), or metanephric (modified and differentiated).
- The structural and functional unit of the kidney is the nephron. It is where the urine is synthesised. 8- The different steps of urine formation, i.e., ultrafiltration, selective reabsorption, and tubular secretion, take place within the different parts of the nephron.
- The urine is a slightly yellowish, acidic fluid, that has a characteristic pungent odor and is involved in removing the nitrogenous and non-nitrogenous wastes from the body.
- The concentration of different constituents of urine varies according to different conditions of the body.
- The countercurrent mechanism regulates the proper concentration of water, several ions in blood and urine.
- The process of release of urine from the body is called micturition.
- Urine formation is also responsible for maintaining osmotic concentration of the blood and other body fluids. This process is called osmoregulation.
- A disease, named Bartter syndrome, is developed due to the absence of a channel protein called Barttin, present within the thick ascending loop of Henle. As a result, reabsorption of ions does not take place, which severely impairs water reabsorption in collecting ducts. Thus, liquid content of the body decreases.
- The functioning of the kidney is regulated by the juxtaglomerular apparatus (JGA), atrial natriuretic peptide (ANP), and antidiuretic hormone (ADH).
- About 2/3rd to 7/8th fraction of glomerular filtrate gets reabsorbed in the PCT, by passive absorption. This process is called obligatory water reabsorption Some amount of water reabsorption takes place in the DCT, due to the effect of ADH. This process takes place by active absorption. This process is called facultative water reabsorption.
- Hyposecretion of ADH causes diabetes insipidus.
- The accessory excretory organs include skin, lungs, liver, salivary glands, et
- Some of the disorders related to excretion include Uremia, nephritis, renal failure, etc.
- Renal calculi or kidney stones is another disorder related to the excretory system.
- Dialysis and kidney transplantation are important procedures involved in the treatment of these diseases.
- In the case of diseases like multiple myeloma, leukemia, lymphosarcoma, etc., a different globulin-type protein is found in the urine. These proteins are known as Bence-Jones proteins.
- The amount of any substance that is released through the urine per minute, is also present in the plasma. The amount of plasma in which this amount of substance is present is known as plasma clearance.