
Cardiac Output
Cardiac Output Definition: Cardiac output is the volume of blood pumped by each ventricle per minute.
Cardiac output depends on the frequency of heartbeat as well as the volume of blood ejected in one contraction.
It is expressed as minute volume or litres of blood per minute. The usual values of cardiac output for adults when at rest are 5 to 6 L/min or approximately 8% of body weight per minute.
With strenuous activity, an adult’s cardiac output can increase to almost 25 L/min to satisfy the body’s demands for nutrients and oxygen. Cardiac output is a product of heart rate (beats/ minute) and stroke volume.
Read and Learn More Class 11 Biology Notes
The amount of blood pumped by each ventricle with each heartbeat is called stroke volume.
In a healthy adult at resting condition, the stroke volume is 70 ml of blood. Cardiac output is calculated by the formula— Cardiac Output (CO) = Stroke Volume (SV) x Heart Rate (HR) So, the cardiac output is 70 x 72 = 5040 ml min’1 or approximately 5 litres min’1.
cardiac output definition
The cardiac output represents the volume of blood that is delivered to the body. It is an important factor in the determination of the effectiveness of the heart to deliver blood to the rest of the body.
“WBCHSE class 11 biology notes for cardiac output”
Cardiac Index And Stroke Volume Index
Normal, resting cardiac output differs among individuals. Therefore, in clinical practice, measured values for cardiac output are often expressed as a flow (L/min) per body surface area (m2) which is called cardiac index.
It is the volume of blood released by each ventricle of the heart per minute to the body surface.
The surface area is estimated from calculations based on body weight and height. Cardiac index normally ranges from 2.6 to 4.2 L/min/m2.
| Class 11 Biology | Class 11 Chemistry |
| Class 11 Chemistry | Class 11 Physics |
| Class 11 Biology MCQs | Class 11 Physics MCQs |
| Class 11 Biology | Class 11 Physics Notes |
The stroke volume index is the volume of blood released during each heartbeat with respect to the surface area of the body. The average value of stroke volume index in a healthy adult human is 47ml.
In 1870, German physiologist Adolf Fick contrived the first method for measuring cardiac output in animals and human beings.
” cardiac output formula”
The basis of this method is called Fick’s principle. This principle states that the amount of any substance received by an organ per unit of time is equal to the arterial level of the substance minus the venous level times the blood flow.
So Blood flow through an Organ In a given time =
Amount of substance removed from or added to blood during the same time period/ A- V difference of concentration of the substance/ml. of blood.
“detailed explanation of cardiac output for class 11 WBCHSE”
Over the past decades, many methods for cardiac output measurement have been developed like thermodilution method, oesophageal Doppler method, transoesophageal echocardiography, pulse contour cardiac output, lithium dilution cardiac output measurement, etc.
factors affecting cardiac output
Factors Controlling Cardiac Output
Maintaining and regulating cardiac output is one of the most intricate functions of the circulatory system.
The cardiac output is the product of stroke volume and heart rate. Therefore, factors regulating stroke volume and/or heart rate are able to control it.
The key factors regulating cardiac output are given below—
Sympathetic stimulation: Increased sympathetic stimulation (due to fright, anger, etc.) increases the heart rate. It also increases stroke volume by increasing contractility, which results in a more complete ejection of blood from the heart.
Hence, cardiac output increases which is again brought to normal by increased parasympathetic activity after sympathetic stimulation.
Venous return: Cardiac muscle fibres are stretched by increased blood volume returning to the heart.
“factors affecting cardiac output in human circulatory system”
Increased stretch results in a greater force of contraction, which increases stroke volume and thereby cardiac output. Decreased venous return decreases cardiac output.
Heart rate: Increased heart rate decreases stroke volume but increases cardiac output. Excessive increase in the heart rate decreases cardiac output.
Myocardial contractility: Increased myocardial contractility results in increased cardiac output.
The strength of the force of myocardial contraction depends on the initial length of cardiac muscle fibres, nutrition and availability of oxygen, concentration of H+ ions, etc.
Peripheral resistance:
- The pressure against which ventricles pump blood is called afterload.
- This is determined by the resistance of arterioles to blood flow, which is called peripheral resistance.
- Increased peripheral resistance will reduce the volume of blood flow through the arteries and will in turn increase afterload.
- This will lower the stroke volume and thereby decrease cardiac output. Thus, peripheral resistance is inversely proportional to cardiac output.
Exercise: Exercise activates the sympathetic nervous system, increasing heart rate and contractility of the myocardium. Both of these actions increase venous return, contributing to increased stroke volume. Hence, cardiac output is increased.
Blood pressure
Blood pressure can be defined as the lateral pressure exerted by the flowing blood on the walls of the blood vessels (especially the arteries).
Types of blood pressure are—
Systolic blood pressure: The peak value of pressure exerted by the blood on the walls of the arteries during ventricular contraction or systole, is known as systolic blood pressure. Normal systolic blood pressure in an adult is in a range of 105-135 mm Hg (average 120 mm Hg) during each cardiac cycle.
“factors affecting stroke volume “
Diastolic blood pressure: The minimum pressure exerted by the blood on the walls of the arteries during ventricular relaxation or diastole, is known as diastolic blood pressure. Normal diastolic blood pressure in an adult is about 80mm Hg (60 – 90 mm/Hg).
Pulse pressure: The term pulse refers to the alternating surges of pressure (expansion and then recoil) in an artery that occurs with each contraction and relaxation of the left ventricle. This difference between systolic and diastolic pressure is called pulse pressure.
“how to calculate cardiac output with formula and examples”
Normally the pulse pressure is SBP-DBP = (120-80)= 40mm Hg.
Mean arterial pressure: Mean arterial pressure (MAP) is the average pressure during the cardiac cycle. The value of MAP varies at different levels of the circulatory system.
Blood pressure can be measured directly or indirectly
Direct measurement of blood pressure is done by cardiac catheter with the help of a pressure transducer or by putting a needle in an artery and connecting with a pressure transducer or simply a Hg manometer.
Indirect measurement of blood pressure involves auscultatory palpatory or oscillatory method by using a sphygmomanometer.
commonly called a blood pressure cuff, is an instrument used to obtain blood pressure readings by the auscultatory method.
Electrocardiogram [ECG]
Electrocardiogram Definition: The electrocardiogram (ECG) is a graphic representation of the electrical activity of the heart recorded during the cardiac cycle.
Discovery: In 1887, Augustus D Waller recorded the first electrocardiogram. After that in 1903, Willem Einthoven studied the details of ECG and he is known as the father of ECG. After 1930, many advanced forms of ECG have been developed.
Description: The electrical activity of the heart is monitored and recorded on the ECG. The process of recording ECG is known as electrocardiography. An ECG configuration may consist of waves, and intervals recorded as voltage against time. A single waveform begins and ends at the baseline.
“difference between stroke volume and cardiac output notes”
Electrocardiograph
Cardiac impulse, generated from the SA node, is transported to all tissues of the heart as electrical impulse via the AV node, a bundle of His, Purkinje fibre, etc., and all over the body through cells and blood.
So, the electrical activity of the heart can be observed by using electrodes at different parts of the body. The instrument used to measure these activities is known as electrocardiograph.
Einthoven’s triangle
During electrocardiography, an imaginary triangle is formed with three limb leads or electrodes (two shoulders and one left leg) by keeping the heart at the centre. This is known as Einthoven’s triangle
Methods of ECG recording: There are various methods for ECG recording. The electrodes that are used for the procedure, are placed in different parts of the body. Generally, there are two types of methods for electrocardiography—unipolar and bipolar ECG methods.
Waves Of Electrocardiogram
The ECG recorded on graph paper is composed of five types of waves— P, Q, R, S and T.
The P wave: The normal cycle of electrical activity in the heart begins with atrial depolarisation and is recorded as the P wave.
The shape of the P wave is usually symmetrical and upright. The normal duration of the P wave is 0.08 to 0.11 seconds.
The QRS complex: The QRS complex represents ventricular depolarization.
“importance of cardiac output in blood circulation WBCHSE notes”
The QRS complex consists of three separate waveforms—
Q wave, R wave, and S wave. The first negative deflection (below the baseline) after the P wave is the Q wave.
The next tall positive deflection (above the baseline) is the R wave. The S wave is the small negative deflection (below the baseline) that follows the R wave. Under normal conditions, the duration of the QRS complex is less than 0.10 seconds.
The ST segment: The ST segment represents the time between ventricular depolarization and repolarization.
It begins at the end of the QRS complex (called the J point) and ends at the beginning of the T wave. Normally, it measures 0.12 seconds or less.
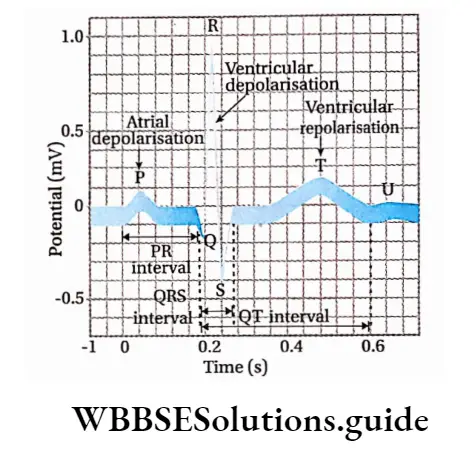
The T wave: The T wave represents ventricular repolarization, rest, and recovery. Its duration normally measures 0.20 seconds or less.
T waves are sensitive T indicators for the presence of a number of abnormalities.
The U wave: The U wave follows the T wave and has the same polarity (deflection) as the T wave. Its origin and mechanism are not known. Due to its low voltage, it is usually flat and almost not visible.
The PR interval: The PR interval starts at the beginning of the P wave and ends at the beginning of the QRS complex.
The normal duration of the PR interval is 0.12 to 0.20 seconds. The PR interval represents the total atrial (supraventricular) electrical activity prior to the activation of the bundle of His, ventricular branches, and Purkinje fibre system.
The QT interval: The QT interval is measured from the beginning of the QRS complex to the end of the T wave.
“heart rate, stroke volume, and their role in cardiac output”
The QT interval represents total ventricular activity. The normal QT interval measures about 0.38 seconds and varies in males and females and with age.
Significance Of ECG
Electrocardiography is an indispensable tool in the diagnosis, prognosis and therapeutic aspect most of cardiac disorders.
From the ECG tracing, the following information can be determined—
- Heart rate and heart rhythm,
- Conduction abnormalities,
- A prior heart attack,
- Chances of coronary artery disease,
- Abnormal thickness of heart muscle.
An electrocardiogram captures the electrical activity of the heart, so it can give information about the following conditions—
- Myocardial Infarction,
- Re-entry pathways in the electrical system,
- Location of the heartbeat initiator, types of cardiac arrest (ventricular fibrillation, a systole, etc.) and other different changes in the electrical activity of the heart.
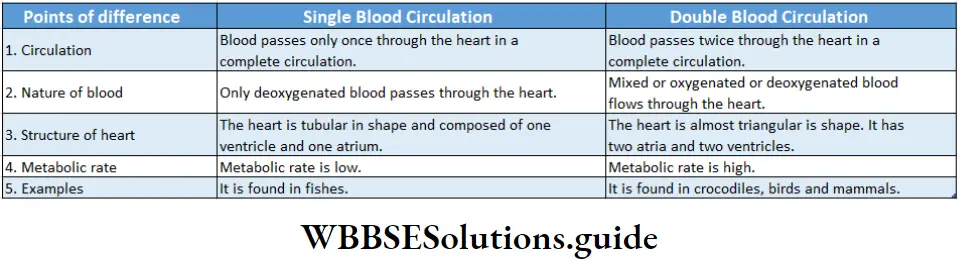
Double Circulation
Double Circulation Definition: When pathways, blood flows through called double the heart circulation.
Double circulation involves the movement of blood through the heart twice during each trip of the body.
The two pathways involved in this area—
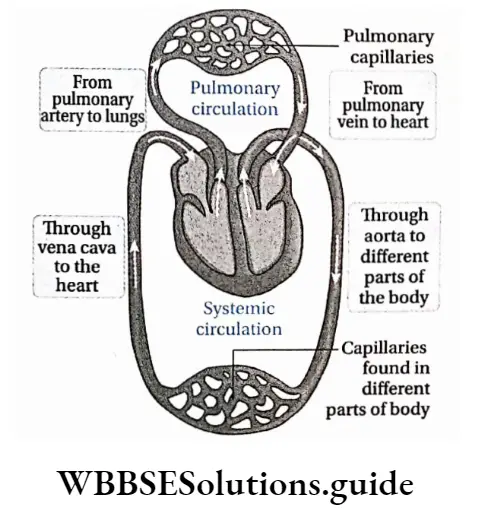
Pulmonary circulation (i.e., transportation of blood from the heart to the lungs) and systemic circulation (i.e., transportation of blood from the heart to the rest of the body).
A double circulation must have a three or four-chambered heart. The right side of the heart receives deoxygenated blood from all over the body and pumps it to the lungs.
In the lungs, the blood loses CO2 and receives O2. The left side of the heart receives oxygenated blood from the lungs and transports it to all the body parts.
Amphibians, reptiles, birds and mammals have double circulation. Fishes have two-chambered hearts. They have a single circulation pathway.
Mechanism Of Double Circulation
The double circulation in human beings can be divided into— pulmonary circulation and systemic circulation.
Pulmonary Circulation
Pulmonary Circulation Definition: Pulmonary circulation is the movement of blood from the heart to the lungs, and then from the lungs back to the heart again. The pulmonary system begins with the pulmonary trunk and ends in the left atrium.
Pathway of circulation:
The pulmonary trunk originating from the right ventricle, divides into right and left pulmonary arteries which enter the right and left lung respectively.
These pulmonary arteries carry deoxygenated blood and divide into smaller arteries, arterioles and capillaries around the lung alveoli.
After gaseous exchange, oxygenated blood from the alveolar capillaries is carried by four pulmonary veins to the left atrium.
Systemic circulation
Systemic circulation Definition: The circulation, in which blood flows from the left ventricle to the body and again returns to the right atrium is known as systemic circulation.
Pathway of circulation:
The aorta originates from the left ventricle and then forms the arch of the aorta. It moves through the lungs as the dorsal aorta. This dorsal aorta crosses the diaphragm and moves into the abdominal cavity. Here, it is known as the abdominal aorta.
The aorta divides into many branches which form capillaries to supply oxygenated blood to different parts of the body.
The visceral capillaries join together to form venules and veins.
Veins combine together and form two main veins—superior vena cava and inferior vena cava. They drain deoxygenated blood into the right atrium from the visceral capillaries.
Regulation Of Cardiac Activity
Cardiac activity in humans is regulated mainly by—neural control and hormonal control.
Neural control: Neural control of the cardiovascular system involves two nerve centres— the cardioinhibitory centre (located in the medulla oblangata of the brain) and the cardioacceleratory centre (located in the vertebral column).
Parasympathetic nerves in the brain and sympathetic nerves in the spinal cord are involved in this regulation.
Stimulation of parasympathetic nerve fibres originating from the cardioinhibitory centre reduces heart rate and blood pressure. This nerve fibre is known as the vagus nerve or 10th cranial nerve.
This nerve fibre is distributed in the SA node, AV node and atrial muscles. Stimulation of sympathetic nerve fibres originating from the cardio accelerator centre of the spinal cord increases heart rate, blood pressure and contractility of cardiac muscles.
These nerve fibres are distributed in the SA node, AV node and the cardiac muscles.
Baroreceptors are a type of sensory neurons that are excited by the stretch of the blood vessel or increase in blood pressure.
They are present in different parts of the body. Due to their stimulation, the produced nerve impulse moves to the brain through the nerves.
As a result, the impulses from the cardioinhibitory centre come to the heart through the vagus nerve. This, in turn, reduces heart rate.
“short notes on cardiac output for WBCHSE class 11 exams”
Hormonal control: Various hormones play a role in the control of the cardiovascular system.
Important sites of hormone secretion include the adrenal medulla, posterior pituitary gland, kidney, and atrium of the heart.
The major hormonal role is played by epinephrine and norepinephrine. Other hormones such as thyroxine, arginine, vasopressin and erythropoietin have some effect on the cardiovascular system.
Atrial muscle cells produce atrial natriuretic peptide which plays an important role in this.
Epinephrine and norepinephrine: When the sympathetic nervous system is activated, the adrenal medulla releases epinephrine (>90%) and norepinephrine (<10%), which circulate in the blood.
Epinephrine and norepinephrine have similar direct effects on the heart, but norepinephrine elicits a powerful baroreceptor reflex because it causes systemic vasoconstriction and increases mean arterial pressure.
Myogenic heart
- A myogenic heart is capable of generating an action potential, depolarization and consequent contraction from within the muscle itself instead of receiving any stimulus from a nerve.
- A healthy heart will perform myogenic rhythms that will allow it to beat 60 to 100 times per minute. Myogenic heart is found in animals like molluscs and vertebrates.
Neurogenic heart
The neurogenic heart refers to the highly specialized muscle cells that require neural input to initiate and maintain contractions. The neurogenic heart is found in animals like annelids and arthropods.
Atrial natriuretic peptide (ANP): Atrial natriuretic peptide is a 28-amino acid polypeptide synthesised and stored in the atrial muscle cells. They are released into the bloodstream when the atria are stretched. It decreases blood volume by increasing sodium excretion.
Other hormones: Thyroxine hormone directly affects the SA node of the heart and increases the heart rate.
Arginine vasopressin (AVP) exerts its major effect on the cardiovascular system by causing the retention of water by the kidneys, which regulates blood volume. Erythropoietin regulates RBC synthesis by stimulating bone marrow.
The decrease in hematocrit stimulates its release, which stimulates RBC synthesis.
Therefore, the increase in plasma volume is balanced with a larger RBC mass.
Disorders Related To Cardiovascular System
There are different types of abnormalities found in the function of the heart and in the circulation of blood.
Hypertension or high blood pressure
Hypertension is a transitory or sustained elevation of both the systemic and pulmonary arterial blood pressure to a level that induces cardiovascular damage.
If the blood pressure lies between 120/80 mm Hg and 139/89 mm Hg, it is called prehypertension (to denote increased risk of hypertension).
A blood pressure of 140/90 mm Hg or above is considered as hypertension.
Cause: Though the exact causes of hypertension are usually unknown, there are several factors including smoking, obesity, lack of physical activity, sedentary lifestyle, etc., which may be responsible for this condition.
Types of hypertension: There are two broad categories of hypertension—
Primary or essential hypertension and Secondary hypertension.
Primary hypertension: It may develop as a result of environmental or genetic causes. It accounts for 90% of the total cases.
It is further divided into two types—
Benign or chronic hypertension: In this condition, blood pressure is usually higher than normal over a long time.
It increases the risk of heart attack, stroke, heart failure, or kidney disease.
Malignant or accelerated hypertension: It is caused by extremely high blood pressure. Immediate medical attention is required in malignant hypertension as it can quickly cause serious damage to the eyes, kidneys and brain.
Causes of malignant hypertension include any form of secondary hypertension, complications of pregnancy, use of cocaine, monoamine oxidase inhibitors (MAOIs), oral contraceptives, etc.
Several diseases such as cerebral oedema, and heart failure can be caused by this condition.
Malignant hypertension can be treated by using medicines such as anti-hypertensive drugs.
Secondary hypertension: High blood related to any other disorder or cause is known as secondary hypertension.
Diabetes, renal disease, renovascular hypertension, Cushing’s syndrome, obesity, and hormonal disorders are some common conditions related to secondary hypertension. Secondary hypertension can also occur during pregnancy.
Effects of hypertension: Most people with high blood pressure have no signs or symptoms. Although a few people with early-stage high blood pressure may experience dull headaches, dizzy spells, etc. Hypertension mainly destroys the heart, kidney, blood vessels and brain.
Effect on heart: Hypertension increases the rate and intensity of the contraction of the heart. This may increase the chances of ventricular hypertrophy and failure. It can also increase the risk of clotting of blood in the lungs and ischemic heart diseases. This affects the circulation of blood and O2 in the body.
Effect on brain: Hypertension may cause haemorrhage, stroke, paralysis and ultimately death.
“WBCHSE class 11 biology human heart and cardiac output notes”
Effect on kidney: Hypertension causes high blood pressure in the kidneys. As a result, the renin-angiotensin system activates and ultimately causes kidney failure.
Prevention and treatment:
- This can be mainly prevented by changing lifestyle.
- It can also be prevented by avoiding the consumption of fatty food, cigarettes, alcohol, etc.
- The patient should take anti-hypertensive drugs.
Mainly, two types of medicines are used in case of hypertension—
Vasodilator drugs: These drugs increase the blood flow to the kidneys. This results in the elimination of excess water, thereby reducing blood pressure (by reducing blood volume).
“cardiac output class 11 WBCHSE PDF notes download”
Natriuretic or diuretic drugs: These drugs decrease the absorption of salt and water in the renal tubules and reduce blood pressure.
Hypotension
Abnormally low arterial blood pressure is known as hypotension. For an adult, less than 90 mm Hg systolic pressure and less than 60 mm Hg diastolic pressure describes hypotension.
Hypotension may result in loss of consciousness, nausea, fatigue, lightheadedness, dizziness, abnormalities in blood circulation, etc.